Published on
John DesMarais, MD and Samidha Dutta, DO
Urgent message: Screening patients with suspected DVT using the Well’s criteria is an efficient tool that would be even more impactful with access to point-of-care, high-sensitivity D-dimer testing in the urgent care setting.
Citation: DesMarais J, Dutta S. Urgent care diagnosis and management of deep vein thrombosis. J Urgent Care Med. 2021;15(2):13-17.
Case Presentation
A 37-year-old woman presents to urgent care with 3-day history of right leg swelling and pain. Her symptoms started without any history of trauma. She denies prior similar episodes. Her symptoms have persisted despite using ibuprofen, warm compresses, and massage to the area. She has pain with ambulation. Her past medical history includes hypertension for which she takes only lisinopril. She denies smoking tobacco or using illicit drugs and drinks alcohol only on holidays. She otherwise lives a very active lifestyle.
On exam, her right calf is warm and erythematous. Palpation of the posterior calf elicits pain. There is nonpitting edema. The right calf is 1 cm greater in diameter compared with the left. The remainder of her exam is unremarkable. Her vitals are normal. She seems uncomfortable when trying to ambulate on the leg but is otherwise in no acute distress.
INTRODUCTION
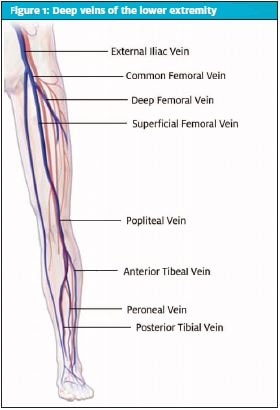
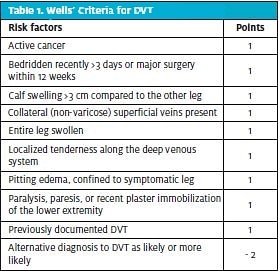
A deep vein thrombosis (DVT) can occur in any of the deep veins [Figure 1]. According to the American Heart Association, it is the third most common vascular diagnosis following myocardial infarction and stroke and affects roughly 300,000 to 600,000 Americans annually.1 While upper extremity DVT can occur, DVTs most commonly involve clot formation in the large veins of the lower extremity and can be classified based on anatomy as either proximal or distal to the knee. A pulmonary embolism (PE) occurs when the thrombus dislodges and travels proximally through the venous system into the pulmonary vasculature. The risk of DVT increases by 60% in individuals over 70 years of age. Approximately half the individuals with untreated proximal DVT develop symptomatic PE within a period of 3 months and 25% of these symptomatic cases result in sudden death.2 The diagnostic test of choice for DVT is venous ultrasound. Unfortunately, this modality is often not readily available in the urgent care or primary care setting; thus, diagnosis is heavily reliant on history, physical exam, and risk stratification to determine when and how rapidly testing should occur. An important risk stratifying tool is the Well’s score for DVT (Table 1). Distinguishing between “provoked” and “unprovoked” and “first-time” vs “recurrent” DVT is critical, as this information has important implications for formulating management plans.
RISK FACTORS
There are many modifiable and nonmodifiable risk factors for DVT. The highest risk of DVT in females occurs before 50 years of age. In males, DVT occurs more commonly over 65 years of age.3 Other nonmodifiable risk factors include the presence of inherited thrombophilias such as Factor V Leiden mutation, prothrombin gene polymorphism, protein C and S deficiency, non-O blood groups, and methylenetetrahydrofolate reductase (MTHFR) gene polymorphism, with the risk greatest in those who are homozygous for these conditions.2,3 The most potent of these genetic risk factors are protein C and S deficiencies, which are present in approximately 15% of patients under the age of 45 who present with a DVT. Deficiency in either of these proteins can increase risk of DVT by 10-fold or more.2
Factor V Leiden mutation, the most prevalent of these genetic conditions, is associated with a lifetime incidence of DVT of about 6.3%.3
Thrombophilias should be suspected in patients with history of recurrent DVT or recurrent miscarriages. Furthermore, family history of thrombophilias in first-degree relatives is also an important component of history-taking in patients presenting with signs and symptoms of DVT.
Acquired and Persistent Factors
The risk of DVT events is several times higher in patients with congestive heart failure (CHF) under the age of 40 compared with those over age 80. Patients with CHF have increased venous stasis resulting from decreased cardiac output and patient immobility. Increasing severity of heart failure is directly correlated with an increased incidence of DVT.2
The overall risk of DVT in patients with advanced cancer increases by seven-fold when compared with the general population.2 Certain cancers such as non-Hodgkin lymphoma, lung, ovarian, brain, pancreatic, and gastrointestinal have higher rates of associated DVT.2 Chemotherapeutic agents such as 5-fluorouracil, tamoxifen, and cisplatin are all medications that influence factors such as hypercoagulability, endothelial injury, and/or blood flow which in turn also contributes to the increase risk of DVT in patients with cancer.2
Several other acquired risk factors include acute infection, chronic inflammatory diseases (eg, systemic lupus erythematosus, rheumatoid arthritis), chronic obstructive lung disease, chronic kidney disease, recent history of stroke (with an increased incidence of DVT by 15% in patients within the first 3 months post-stroke), recent major surgery (especially orthopedic surgeries), and trauma (eg, spinal cord injuries).2,3
DVT risk increases in a dose-dependent manner in response to estrogen levels, especially in patients on hormone-replacement therapy or taking combination oral contraceptives. Similarly, later stages of pregnancy and the puerperium period also increase the risk of DVT by a rate 1.4%.3 This relation is also the understood mechanism for why premenopausal women, ie, those under the age of 50, have a higher incidence of DVTs.
Modifiable risk factors
Modifiable risk factors include obesity, increased waist circumference, and cigarette smoking. Obese individuals are overall twice as likely to develop DVT.2 Patients with childhood obesity maintain an increased risk of DVT into adulthood even if their BMI normalizes.4 Metabolic disorders such as diabetes are also included in these modifiable lifestyle-related risk factors; other modifiable risk factors include immobilization, dehydration, and long-term steroid.2,3
DIAGNOSIS
DVT can present with unilateral leg pain, swelling, and occasionally redness of the affected extremity. Many times, however, the nonspecific nature of the patient’s complaints necessitates the use of objective tests to confirm a diagnosis.
D-dimer is among the most common and widely available screening tests for DVT and PE. D-dimer is a fibrin clot degradation product which is increased in patients with both acute and chronic thrombosis. Unfortunately, although very sensitive, its use is limited as a stand-alone test because of its low specificity, resulting in frequent false positive results. Many conditions, such as recent surgery, trauma, pregnancy, older age, and cancer can lead to d-dimer elevation.4 Because of the low specificity, assessing pretest probability is often combined with d-dimer assay testing to improve diagnostic capability.
Interpretation of the Wells’ Score
The Wells’ DVT risk score is a widely used and validated clinical decision tool used to help determine the pretest probability of DVT.3 A score of 0 represents a 5% risk of DVT. A score of 1–2 represents a 17% risk and 3 or greater is associated with a 17% to 53% prevalence risk. Patients with the lowest Wells’ score (-2), however, still have up to a of 5% risk of thrombus, underscoring that DVT cannot be 100% excluded using the Wells’ score alone.3 The current recommendations favor a combined approach toward diagnosis: Patients with a score of 1 or less on the Wells’ criteria have a low risk of DVT, so this should prompt a D-dimer test which, if negative, can reliably exclude the diagnosis. If the d-dimer is positive in these cases, a confirmatory diagnostic imaging test should follow. Patients who have a high-risk Wells’ score of 2 or more do not need a d-dimer but may proceed immediately to a diagnostic imaging test to confirm the diagnosis.7
D-dimer levels increase with age, leading to even lower specificity for DVT in older patients. An age-adjusted d-dimer threshold, defined as the patient’s age multiplied by 10 ng/mL, has been suggested for patients older than 50 years.4 This age-adjusted strategy improved specificity by about 9.5% from 45.2% to 54.7% and reduced false positives to a more acceptable level.3,5
In outpatient settings, the preferential diagnostic imaging choice should be venous compression ultrasound. Alternative imaging modalities like venography, CT, and MR venography can be utilized; however, this is a less desirable approach due to high cost, exposure to ionizing radiation, reaction to contrast media, or their invasive nature.
DIFFERENTIAL DIAGNOSIS
- Distal DVT – The ultrasound may demonstrate a distal DVT in one of the calf veins. Anticoagulation is controversial in these settings unless the patient has risk factors for extension (eg, an unprovoked DVT or previous venous thromboembolism) or develops extension on serial ultrasound exam, which should be done 2 to 3 weeks after the initial diagnostic investigation to exclude propagation of the clot.
- Severe calf muscle pull/trauma – The history usually involves an injury, and there are usually signs of bleeding on the ultrasound or hematoma formation or bruising at the ankle.
- Superficial thrombophlebitis – This classically presents as tender hard or red-appearing swollen superficial veins. Superficial thrombophlebitis may be associated with DVT and should be further evaluated with venous ultrasound.3
- Cellulitis – Cellulitis, like DVT, causes warmth, swelling, and redness of an affected extremity. Furthermore, the two conditions can co-exist and, therefore, ultrasound may be necessary in such presentations.
- Lymphedema –– This is a cause of chronic edema. Since there are no distinguishing factors between lymphedema and edema associated with DVT, ultrasound is generally appropriate when there is acute increase in swelling or pain.
- Popliteal (Baker’s) Cyst – This is often distinguished from DVT by its presentation as posterior knee pain with knee stiffness and a swollen mass behind the knee. Ultrasound is still often performed nonurgently to confirm the presence of a full or partially drained Baker’s cyst.
- Interstitial edema – Lower extremity edema is commonly found in patients with heart failure, liver disease, or can be associated with medications like dihydropyridine calcium channel blockers (amongst others). The edema in these cases is usually bilateral but can be asymmetric if accompanied by underlying venous pathology. Signs of inflammation are usually not present, and if the Well’s score is low risk and the d-dimer is negative then no further investigations need to be performed.3
TREATMENT
Anticoagulation is the mainstay for management of DVTs with the goal of preventing progression, recurrence, and providing acute relief of symptoms. Management of DVTs can be categorized into an acute phase and a chronic phase. The acute phase typically includes the first 3 to 6 months after onset. Most instances of DVT can be managed on an outpatient basis except in severe cases such as proximal clots (eg, common femoral and/or iliac veins), phlegmasia/limb ischemia, significant comorbidities such as end stage renal disease, and high bleeding risk.6
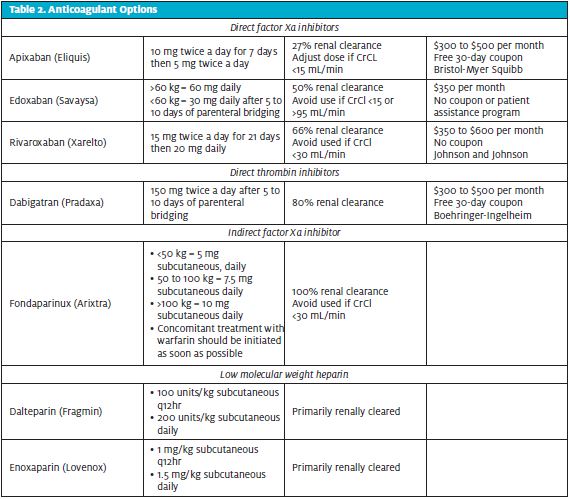
There are several options for anticoagulation, including vitamin K antagonists such as warfarin, direct oral anticoagulants (DOAC), and low- molecular-weight heparin (LMWH) (Table 2), as well as unfractionated heparin. The optimal choice depends on the patient’s comorbidities, renal function, and often financial and practical considerations, as well (eg, dosing frequency and route).
Acute Treatment
Typical options for initial treatment of DVT include the DOAC medications which can, but not necessarily need to, be preceded by parenteral anticoagulation, such as a LMWH. If choosing warfarin, initial parenteral anticoagulation is needed for at least 5 days until INR is greater than 2.0 on two occasions that are 24 hours apart.3 Options for parenteral bridging include heparin derivatives such as LMWH or unfractionated heparin (UFH).
In general, guidelines for anticoagulation recommend DOACs for most non-cancer-related DVTs, especially compared with the alternative oral option of warfarin. Several meta-analyses have demonstrated evidence of lower rates of major and even fatal bleeding with DOACs compared with warfarin.3 Furthermore, compared with warfarin, DOACs have more predictable pharmacokinetics and rapid onset of action. Warfarin also requires frequent blood draws for monitoring of INR.
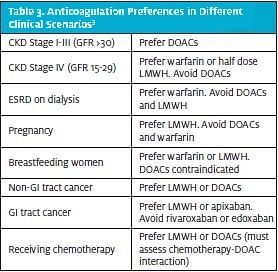
There are special clinical scenarios that warrant use of specific anticoagulants [Table 3]. For example, in a study of 120 high-risk patients with antiphospholipid syndrome, warfarin was shown to have lower rates of thromboembolic events compared to rivaroxaban.3 In the instance of cancer, LMWH is the standard of treatment. When compared with DOACs, LMWH has lower rates of major bleeding due to gastrointestinal events. However, in non-GI cancers, DOACs are considered an acceptable alternative to LMWH, showing noninferior effects on bleeding risks and, occasionally, even lower rates in recurrence.3
In the acute phase, isolated proximal DVTs are usually managed with 3 to 6 months of anticoagulation. If the isolated DVT occurs distally in calf, management options include a shorter course of 4 to 6 weeks or even serial compression ultrasonography without starting anticoagulation for monitoring propagation of the clot.10
Chronic Treatment
Extension of treatment after the first 3 to 6 month usually depends on stratification based on risk of recurrence. The risk of recurrence is >3% in individuals with active cancer, active autoimmune disease, or antiphospholipid syndrome. For such patients, it is recommended to annually assess their risk of DVT and need for anticoagulation. Provoked DVTs also fall under this category of long-term anticoagulation; however, the characterization of provoked vs unprovoked DVTs is no longer used to determine length of treatment due to presence of predisposing factors. Postthrombotic syndrome or venous insufficiency occurs in 25% to 50% of patients at 3 to 6 months after diagnosis.3 In cases such as trauma resulting in fractures, minor surgery with anesthesia for more than 30 minutes, or acute illness resulting in immobility for more than 3 days, prolonged anticoagulation therapy is not warranted.3
Case Conclusion
The Wells’ score is applied, and this patient gets 1 point for her pain along the deep venous system. Based on this, the patient has moderate risk with a 17% pretest probability.7-9 Per current recommendations, the next step would be to complete a high-sensitivity D-dimer blood test. The patient has a negative high-sensitivity D-dimer testing completed in the urgent care. In moderate-risk patients with a negative high-sensitivity D-dimer by point-of-care testing, DVT can be ruled out with a negative predictive value of 96.1% and no further testing.7-9 The patient is safely sent home with primary care follow-up.
Unfortunately, most urgent care settings do not have rapid D-dimer testing available on site. Having point-of-care high-sensitivity D-dimer testing in urgent cares would be beneficial in preventing delay of care, diagnostic uncertainty, and associated costs.
REFERENCES
- What is venous thromboembolism? https://www.heart.org/en/health-topics/venous-thromboembolism/what-is-venous-thromboembolism-vte. Published March 1, 2017. Accessed July 23, 2021.
- Phillippe, HM. Overview of Venous Thromboembolism. American Journal of Managed Care. https://www.ajmc.com/view/overview-of-venous-thromboembolism. Published December 27, 2017. Accessed July 23, 2021
. - Chopard R, Albertsen IE, Piazza G. Diagnosis and Treatment of Lower Extremity Venous Thromboembolism: A Review. JAMA. 2020;324(17):1765–1776. doi:10.1001/jama.2020.17272
- Phillippe, Haley M. Overview of Venous Thromboembolism. Am J Manag Care. 2017;23: S376-S382
- Horner, Dan. New NICE Guidelines on diagnosis and management of venous thromboembolism. St. Emlyn’s, May 2020, https://stemlynsblog.org/nice-guidelines-vte/
- Cohoon KP, Heit JA. Inherited and Secondary Thrombophilia. Circulation. 2014;129:254–257. https://doi.org/10.1161/CIRCULATIONAHA.113.001943
- Wells PS, Hirsh J, Anderson DR, et al. Accuracy of clinical assessment of deep-vein thrombosis. Lancet. 1995;345(8961):1326-30.
- Wells PS, Anderson DR, Bormanis J, et al. Value of assessment of pretest probability of deep-vein thrombosis in clinical management. Lancet. 1997;350(9094):1795-8.
- Wells PS, Anderson DR, Rodger M, Forgie M, Kearon C, Dreyer J, Kovacs G, Mitchell M, Lewandowski B, Kovacs MJ. Evaluation of D-dimer in the diagnosis of suspected deep-vein thrombosis. N Engl J Med. 2003 Sep 25;349(13):1227-35.
- Wilbur J, Shian B. Deep venous thrombosis and pulmonary embolism: current therapy. Am Fam Physician. 2017;95(5):295-302.
Author affiliations: John DesMarais, MD is program director, Adena Family Medicine Residency. Samidha Dutta, DO, PGY-3 is a third-year resident in theAdena Family Medicine Residency. The authors have no relevant financial relationships with any commercial interests
Read More on DVTs
- Outpatient Management Of Deep Venous Thrombosis
- Case Report: Upper Extremity Deep Venous Thrombosis – Paget-Schroetter Syndrome
- Leg Pain In A 34-Year-Old Man