Published on
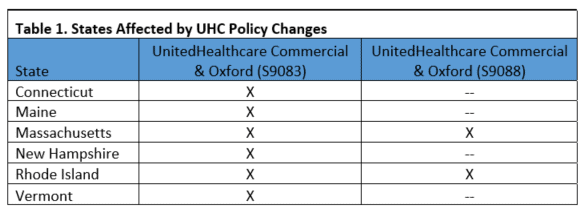
Beginning April 1, 2019 UnitedHealthcare will revise their policies to discontinue reimbursement for HCPCS code S9083, “Global fee urgent care centers” in some states (see Table 1). The change affects UnitedHealthcare commercial plans, United Healthcare Oxford, and UnitedHealthcare Community Plan policies. Additionally, UnitedHealthcare Community Plan will no longer reimburse HCPCS code S9088, “Services provided in an urgent care center.” Providers should report the Evaluation and Management (E/M), and/or procedure code(s) that specifically describes the services provided, consistent with the Current Procedural Terminology (CPT) manual.
Q: Are the 2019 telehealth Healthcare Common Procedure Coding System (HCPCS) codes G2010 and G2012 approved by Medicare restricted to Rural Health Care (RHC) or Federally Qualified Health Care (FQHC) centers?
A: No, these codes are not restricted to RHC or FQHC centers. As of January 1, 2019, providers who can bill an evaluation and management (E/M) service can bill these codes when appropriate, as published in the final rule for the 2019 Physician Fee Schedule (PFS) (https://s3.amazonaws.com/public-inspection.federalregister.gov/2018-24170.pdf). The Centers for Medicare and Medicaid Services (CMS) has agreed to allow separate payment for brief check-in services and remote evaluation of recorded video and/or images that do not result in an office visit, or are not part or a prior office visit. Full descriptions of the new codes are:
- G2010, “Remote evaluation of recorded video and/or images submitted by an established patient (eg, store and forward), including interpretation with follow-up with the patient within 24 business hours, not originating from a related E/M service provided within the previous 7 days nor leading to an E/M service or procedure within the next 24 hours or soonest available appointment”
- National average reimbursement is $12.61
- G2012, “Brief communication technology-based service, eg, virtual check-in, by a physician or other qualified health care professional who can report evaluation and management services, provided to an established patient, not originating from a related E/M service provided within the previous 7 days nor leading to an E/M service or procedure within the next 24 hours or soonest available appointment; 5-10 minutes of medical discussion”
- National average reimbursement is $14.78
Both of these codes can be billed for established patient visits only and a copay is required. CMS has cited the Current Procedural Terminology (CPT) definition of an established patient as one who has received professional services from the physician or qualified healthcare professional or another physician or qualified healthcare professional of the same specialty and subspecialty who belongs to the same group practice, within the past 3 years.
Since CMS did not allow for a process where the patient gives consent once and a copy is kept on file, patient consent must be obtained and documented for each visit of this type. Consent may be oral or written, including electronic confirmation, and must be documented in the medical record for each billed service. In addition, CMS has not given a limit to the number of times these services can be billed, but will monitor utilization of the codes to determine whether limitation should be required in the future. CMS also reminds us that, like all other physicians’ services billed to Medicare, the services must be medically reasonable and necessary to be reimbursed.
These codes are valid for providers only, and cannot be billed by clinical or nursing staff who are not eligible to bill for E/M services. While reimbursement may seem low, CMS believes that it accurately reflects the resources involved in furnishing the service, and provides a valuable service to patients.
HCPCS code G2010, defined as remote evaluation of prerecorded patient information, can only be billed when the patient has submitted a still or video image via asynchronous telemedicine technology. Once the provider has reviewed and interpreted the image(s), a follow-up response must take place within 24 hours. The follow-up can be made with a phone call, audio/video communication, secure text messaging, email, or patient portal communication.
For example, an established patient emails a picture of a rash on his arm and explains that he came across poison ivy while doing yard work, and would like the provider to review the image and confirm whether the rash is poison ivy or not. The provider reviews the image and documents that the rash is consistent with poison ivy, and recommends an over-the-counter ointment, also advising that he should to contact the urgent care center again if there is no improvement. This information is relayed to the patient via secure email. The patient does not require an office visit, nor does he come to the clinic in the next 24 hours, so it is appropriate to bill HCPCS code G2010 for the service.
HCPCS code G2012, defined as virtual check-in, requires direct interaction between the provider and the established patient, whether it be through audio only, real-time telephone interactions or synchronous, two-way audio interactions that are enhanced with video or other kinds of data transmission. CMS was not explicit in descriptions of the technology on purpose, so as not to have to update policies frequently. There are no service-specific documentation requirements aside from documenting the verbal patient consent.
The creation of these new codes exemplifies CMS’s renewed vision to bring the Medicare program into the future of virtual care services and encourages providers to use new technologies to deliver medical care.