Published on
Urgent message: Early diagnosis is crucial in patients with this rare – but potentially fatal – condition, Stevens-Johnson Syndrome.
RACHEL CETTA, BSBE, MSBE, and JOHN SHUFELDT, MD, FACEP
Overview
Stevens-Johnson Syndrome (SJS) is a rare and potentially life-threatening condition. While the exact etiology is unclear, SJS often is associated with an adverse drug reaction to an assortment of drugs ranging from nonsteroidal anti-inflammatory drugs (NSAIDs) to anticonvulsants.1 SJS involves blistering and sloughing off of necrosed skin, leaving a burn-like appearance.
Mucous membranes are also widely affected. SJS typically affects about 10% or less of the skin surface. The main characteristics include delayed hypersensitivity and immunologic processes.2 SJS can occur at any age but it is more common in patients ages 25 to 47 and generally seen in the spring and winter.3 Depending on the extent of skin involvement, it may be necessary to treat an SJS patient as you would someone with a burn.4
Case Presentation
A 41-year-old woman with a history of systemic lupus erythematous (SLE) being treated for a urinary tract infection with Bactrim (sulfamethoxazole and trimethoprim) presents with a diffuse, erythematous rash, pruritis and chills.
Nine days earlier, she presented with dysuria, lowgrade fever and mild flank pain. She was not vomiting. Urinalysis showed 50 to 100 white blood cells (WBCs) and was nitrite-positive. The patient was discharged on pyridium and Bactrim and told to follow up with her primary care physician in 2 days or to return immediately if her symptoms worsened.
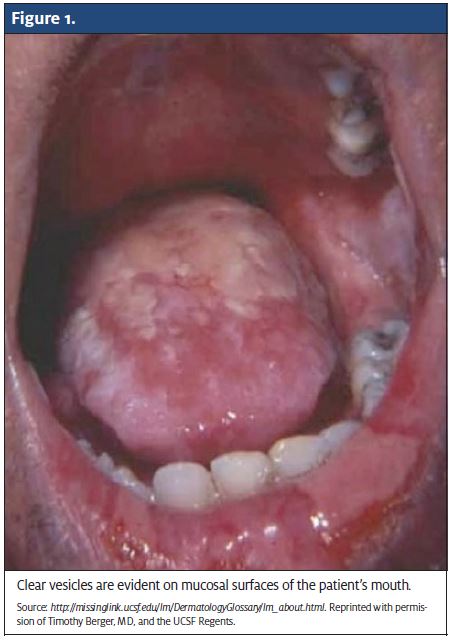
The patient now states that 4 days ago, she began to notice a slight rash and some clear vesicles on the inside of her lower lip. Other than SLE, she has no past medical history. She does not smoke or drink and has no known exposure to atopy.
Physical Exam
- Vitals P: 110
- RR: 18
- T: 38.1°C BP: 108/60
- General: Ill-appearing and in mild distress. HEENT
- PERRL, EOMI, conjunctiva is erythematous. Clear vesicles in the mouth on mucosal surfaces (Figure 1).
- Airway is patent.
Neck: Supple, midline trachea, no overt lymphadenopathy, no meningeal signs.
Lungs: Clear.
Heart: Tachycardic, regular rhythm. GU: No tissue sloughing.
Skin: Erythematous macules with darker, purpuric centers on the chest, back, hands and upper arms (Figure 2). Scattered clear bullea are also noted along with a positive Nikolsky sign.
Labs/Imaging
- CBC: WBC 14,500 with 20% bands, H/H 13/39, Plts 120,000
- UA: Normal save for specific gravity of 1.035
- Chem 7: Normal save for Cr. 1.3
Diagnosis
When a patient presents with diffuse rash in the urgent care setting, it is important for providers to look for the signs and symptoms of SJS.
Important physical exam findings are:
- Fever
- Flu-like symptoms
- Blisters of the mouth, nose, or genitalia
- Conjunctivitis
- History of recently beginning a prescription or over-the-counter1
Some characteristic signs of SJS include:
- Erythroderma
- Skin necrosis
- Blistering and epidermal detachment; and
- Palpable 5
Differential Diagnosis
SJS can be easily misdiagnosed if a patient presents early in the disease course. It also can be mistaken for these other disease processes:
Toxic epidermal necrolysis (TEN): There is discussion about whether TEN and SJS are the same disorder. Some consider SJS and TEN to be the same but of varying severity. Others consider them to be in different categories. By definition, TEN covers over 30% of the body, whereas SJS involves only 10%. If the affected area falls between these two percentages, the classification becomes SJS/TEN overlap syndrome. TEN patients generally present with a higher fever than patients with SJS. TEN is more likely to affect adults in their late 40s or older.3
Erythema multiforme (EM): SJS is sometimes referred to as EM major. However, EM major is considered a separate process because of “targetoid lesions” and lack of mucosal involvement. The herpes virus has a strong connection to EM, while SJS is more likely drug reaction-related.3
Erythematous drug eruption: SJS can resemble erythematous drug reactions early in the course. Erythematous drug eruption differs from SJS because it does not have a mucosal component.3
Toxic shock syndrome (TSS): Patients with TSS have some desquamation about a week after onset on the palms of the hands and soles of the feet. As with SJS, there is mucosal involvement of oropharyngeal mucosa and conjunctiva. TSS is most often caused by Staphylococcus aureus and likely to involve more organ systems than SJS.3
Paraneoplastic pemphigus (PNP): Patients with PNP have oral and ocular mucosal blisters and skin lesions similar to EM. PNP can be seen in patients with malignancy or in adults with non-Hodgkin’s lymphoma.3
Course and Treatment
First and foremost, immediately stop administration of the drug suspected of causing SJS. In our patient’s case, Bactrim was stopped. Some of the more common drugs that lead to SJS are anti-gout medication (allopurinol), antipsychotics and anticonvulsants (carbamazepine, lamotrigne, phenobarbital), antibiotics (sulfonamides and penicillins),3 TNF-a. antagonists (infliximab and adalimumab), and oxicam NSAIDS (piroxicam and tenoxicam).4
Patients with SJS are considered to “burn from the inside out,” and require copious intravenous fluids and high-calorie nutrition. Pain medication is used to make them more comfortable.1 Mouthwashes can help with oral mucosal damage. Skin wounds are treated similarly to burns, and saline compresses are recommended.4 Silver nitrate can be used as a topical antibiotic. Silver sulfadiazine is not used because SJS is thought to have a connection to sulfonamides.5
When handling SJS patients, sterile technique is necessary because they are at high risk of infection. If a patient’s condition is severe, admission to a burn unit for expert wound care may be necessary.2
Antibiotics can help prevent sepsis and a high dose may be needed.1 As in burn patients, drug pharmacokinetics may be decreased in patients with SJS.4 Conversely, prophylactic antibiotics are not useful and may lead to super-infections. Instead, antimicrobials should be initiated as soon as an infection is documented. Glu- cocorticoids are suggested for adults if diagnosed within the first 48 hours. Beyond that, glucocorticoids are not advised because of the increased risk of immunocompromise and sepsis. For children, glucocorticoids are not recommended because of the range of side effects.5 Immunosuppressive drugs have not been shown to increase recovery and are not advocated.2
A multitude of sequelae are associated with SJS, including permanent blindness, scarring of mucous membranes, and chronic obstructive pulmonary disease.1 Gastroenterologic and genitorurinary complications such as esophageal strictures and renal tubular necrosis, respectively, also can result. Cosmetic defor- mity is another complication.4 These conditions must be identified so they can be treated as well.
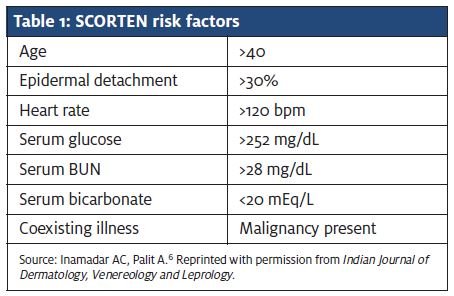
The mortality rate for SJS ranges from 1% to 3%, ver- sus 25% to 35% for TEN.5 The widely used TEN scoring system or SCORTEN also can be used to determine mor- tality in patients with severe SJS based on the risk fac- tors in Table 1.6 Trent et al. found the mortality rate to be 3.2% in patients with 0 to 1 risk factor, 12.2% with 2 risk factors, 35.5% with 3 risk factors, 58.3% with 4 risk factors and 90% in patients with 5 or more risk factors.7
Discussion
A diagnosis of SJS should be considered in patients who present with erythematous skin lesions and mucous membrane involvement and have recently started taking a new medication. The potentially inciting drug needs to be stopped immediately. An adverse drug reaction is the main cause of SJS, but in rare cases, the cause can be vaccination, chemical exposure, or food. In pediatric cases, infections such as the herpes simplex or Epstein-Barr viruses have been known to cause SJS.3,4 HIV-infected patients or those who have certain genetic predispositions are at increased risk of SJS. Many cases are idiopathic.4
Currently there is no specific therapy for SJS. General supportive care is basic procedure. For patients who have rapidly lost epidermis, the re-epithelization process will begin a few days after the sloughing process ceases. The re-epithelization process can be completed within a few weeks.4
Patients with SJS should be educated about the type of drug that caused them to develop the condition. It is important for them to avoid drugs that are similar in structure to the culprit drug and critical that they understand that re-exposure could be fatal.5
SJS is rare, but deadly if not treated in a timely manner. If recognized early enough, though, a patient should survive without significant complications. Unfortunately, there is always a chance for secondary infections that may require long-term antibiotic therapy.
References
- The facts about Stevens-Johnson Syndrome (SJS). Stevens Johnson Syndrome Foun- 2006. http://www.sjsupport.org/pdf/SJS_ factsheet.pdf. Accessed November 6, 2012.
- Gerull R, Nelle M, Schaible Toxic epidermal necrolysis and Stevens-Johnson syn- drome: a review. Medscape. http://reference.medscape.com/medline/abstract/21358399. Accessed November 6, 2012.
- Nirken M H, High W Stevens-Johnson syndrome and toxic epidermal necrolysis: Clincial manifestations; pathogenesis; and diagnosis. UpToDate. http://www.uptodate.com. millennium.midwestern.edu/contents/stevens-johnson-syndrome-and-toxic-epidermal-necrolysis- clinical-manifestations-pathogenesis-and-diagnosis?source=search_result&search= SJS&selectedTitle=2%7E150. Accessed November 6, 2012.
- Foster Stevens-Johnson Syndrome. Medscape. http://emedicine.medscape.com/article/1197450-overview. Accessed Novemer 6, 2012.
- High WA, Nirken Stevens-Johnson syndrome and toxic epidermal necrolysis: Man- agement, prognosis, and long-term sequelae. UpToDate. http://0-www.uptodate.com.millennium.midwestern.edu/contents/stevens-johnson-syndrome-and-toxic-epidermal-necrol-ysis-management-prognosis-and-long-term-sequelae?source=search_result&search=sjs&sele ctedTitle=1%7E150. Accessed November 6, 2012.
- Inamadar AC, Palit Acute skin failure: Concept, causes, consequences and care.
- Indian J Dermatol Venereol Leprol. 2005; 71(6):379-385.
- Trent JT, Kirsner RS, Romanelli P, Kerdel FA. Analysis of Intravenous Immunoglobulin for the Treatment of Toxic Epidermal Necrolysis Using SCORTEN: The University of Miami Experience. Arch Dermatol. 2003;139(1):39-43.
