Published on
THE RESOLUTION
 Differential Diagnoses
Differential Diagnoses
- Pathologic fracture
- Acromioclavicular separation
- Shoulder dislocation
- Pneumothorax
- Pulmonary contusion;
Physical Examination
The patient was afebrile, with a pulse of 103 beats/min, respirations of 16 breaths/min, and a blood pressure of 108/68 mm Hg. He was alert and oriented.
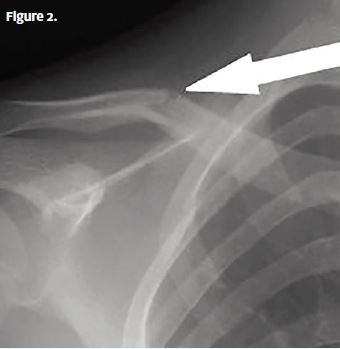
Both lungs were clear to auscultation. His heart rate and rhythm were normal and without murmur, rub, or gallop. His abdomen was soft and nontender, without rigidity, rebound, or guarding. His right shoulder was normal in appearance, without an empty sulcus sign. He had good range of motion of the shoulder, but he winced whenever he moved it. There was a bulge at the mid aspect of the right clavicle and pain with palpation at this site, but there was no evidence of cuts or breaks in the skin. The patient’s neurovascular function was intact, with a normal right radial pulse. A clavicle x-ray was obtained, and it showed a mid-shaft, nondisplaced fracture.
Diagnosis
Right mid-shaft clavicle fracture (Figure 2).
Learnings
Clavicle fractures account for 3.3% of all adult fractures in one study, although those findings may underestimate the frequency, because many of these injuries occur in children. The most common location is the mid aspect of the clavicle (69%–81%), then the distal clavicle, and then—less than 5% of the time—the proximal clavicle. Fractures may be approximated or grossly displaced. As with every evaluation, consider other injuries while taking into account the mechanism of injury, including trauma to the elbow and wrist, head, and neck.
The clavicle approximates medially with the sternum and distally with the acromion. The clavicle provides stability to the upper extremity and protects the deep neurovascular structures:
- Subclavian vessels
- Brachial plexus
- The lung apex
If the mechanism was a fall, there may be other injuries. Inquire about pain in the elbow, shoulder, head, and neck. Differentiate a mechanical fall from a syncopal episode. If there was an altercation, inquire about other injuries and the possibility of abuse. Assess for neurovascular compromise.
The physical examination starts with inspection of the clavicle, because the location of the fracture (proximal, middle, or distal third of the clavicle) will/can usually be approximated on visual inspection alone. Palpate for the area of greatest pain. Assess the range of motion of the shoulder, and document whether lung sounds are symmetric.
An x-ray is the initial test of choice to evaluate for fracture of the clavicle, dislocation of the shoulder, and injury to the lungs when there is any concern for pneumothorax or great vessel injury. Computed tomography and magnetic resonance imaging are rarely needed.
Treatment, even for significantly displaced fractures, is typically initiated with an arm sling, though multiple studies have shown lower rates of nonunion of displaced mid-shaft clavicle fractures with surgical repair. A figure-of-eight splint should not be used, because it results in significantly higher rates of patient dissatisfaction. Pain should be controlled with either hydrocodoneacetaminophen (Vicodin) or oxycodone-acetaminophen (Percocet) with the addition of over-the-counter nonsteroidal anti-inflammatory medications such as ibuprofen. Use caution with older patients.
Emergency department referral should be done immediately with the following:
- Open fractures
- Concerning mechanism of injury such as major trauma from a motor vehicle collision
- Possibility of abuse
- Associated pneumothorax or possibility of great vessel injury
- Unstable vital signs