Published on
Urgent message: Patients presenting to the urgent care center with split earlobe injuries can have their defect repaired with good cosmetic results. This minor office-based procedure can be easily performed in this venue by the urgent care provider.
Oscar D. Almeida, Jr., MD, FACOG, FACS
Dating back to the 2nd Century in the Roman Empire, earrings have remained a staple of human fashion. Today, the popular use of earrings has become gender neutral. The expanded use and differing styles/shapes of earrings have resulted in an increased risk for earlobe injuries.
Split earlobe (lobule) injuries commonly result from the use of large heavy earrings or sudden trauma, including sports injuries or animal bites, such as when an earring gets caught or pulled forcefully. Allowing the defect to heal by secondary intention will lead to a cosmetic deformity.
Given that the earlobe is composed of tough areolar and adipose connective tissues, once a pierced hole from the stress of a heavy earring or trauma, a laceration can occur resulting in earlobe clefting or a bifid earlobe. Since these injuries do not properly heal by themselves and can become infected, expedient wound care and closure will prevent permanent disfigurement of the ear.
The aesthetic goal is to leave the earlobe in a more natural shape with a round, not pointed, shape. The growing accessibility of urgent care centers means this minor office-based procedure can be easily performed in this venue, thus adding another service available to our patients. Although patients may present to our urgent care for other healthcare issues, if we identify a prior split earlobe injury during their visit, repair of this defect can be offered.
Technique
The first step involves proper positioning of the patient. Adolescent and adult patients are placed in the lateral decubitus position with the injured ear facing up. Children under 6 years of age present a positioning challenge. This obstacle can be overcome by using the parental papoose technique,1 in which the child is placed on the parent’s lap, giving them an added level of comfort during the procedure. Cooperation of the child is further enhanced by using a “vocal local,”2 an anesthesia technique which the child is given verbal reassurance by the parent and urgent care provider.
After the patient is properly positioned, a sterile field for the affected ear is created. Using a 27- or 30-gauge needle, local infiltration of the ear is performed using lidocaine 1% or 2% with epinephrine. The use of lidocaine with epinephrine is beneficial for earlobe repairs because it decreases the amount of blood in the field, prolongs anesthesia, reduces the time of the procedure and is supported in the medical literature.3,4
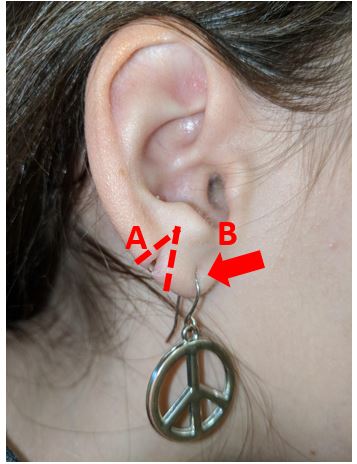
Figure 1. A. Split earlobe caused by heavy earring. Dashed lines outline edges to be excised for repair. B. Note the precursor split earlobe “in progress.”
A full thickness wedge excision of the earlobe defect (outlined in Figure 1A) is performed using a number 11 or 15 scalpel. The resulting fresh surgical margins (Figure 2) are then ready for approximation. The margins are closed with simple interrupted 5-0 or 6-0 nonabsorbable suture, either nylon or Ethilon (Figure 3). Since the earlobe is void of cartilage, skin eversion is not necessary.
Sutures are removed in 7-14 days, leaving a good cosmetic result (Figure 4). The remaining scab generally falls off within 3 weeks. Application of an over-the-counter gel-based product such as Mederma can be used to further improve scar appearance by making the affected skin softer and smoother. Antibiotics may be prescribed for wounds that show signs of inflammation, contaminated wounds, or bite injuries. For best results, patients should wait at least 6 months to re-pierce, doing so at a minimum of 2 mm lateral to the repaired defect. Patients should be counseled in preventive measures to avoid a repeat of the split earlobe (eg, large heavy earrings).

Figure 2.
Fresh surgical margins following wedge excision of the earlobe defect
Figure 3.

Simple interrupted sutures are placed on the surgical margins of the earlobe circumferentially.
Contraindications
Although simple split earlobe repairs can be performed by the urgent care provider, certain injuries of the ear require immediate referral to a plastic surgeon. These include severe crush injuries, complete or near-complete avulsions, auricular hematomas which can lead to cauliflower ear, auditory canal involvement, and wounds requiring removal of greater than 5 mm tissue.

Figure 4. Sutures are removed in 7-14 days. The scab will fall off within 3 weeks.
Billing/Coding
Self-pay costs for split earlobe repair generally range between $400 and $600. Many insurance plans will cover this procedure.
- 2019 ICD-10-CM Diagnosis Code S01.312A: Laceration without foreign body of the left ear, initial encounter.
- 2019 ICD-10-CM Diagnosis Code S01.311A: Laceration without foreign body of the right ear, initial encounter.
Conclusion
Urgent care centers continue to evolve and accommodate the ever-expanding healthcare needs of our patients. Services traditionally performed only in hospitals or specialist offices are starting to migrate to the urgent care setting because of fast service, convenient locations, and affordable pricing. Other examples, in addition to earlobe repair as described here, include allergy testing, concussion evaluation, and many minor surgical procedures such as repair of split earlobes.
References
- Almeida OD Jr. Employing the parental papoose technique in treating young children. J Urgent Care Med. 2018;13(1):26-29.
- Almeida OD Jr, Val-Gallas JM, Browning JL. A protocol for conscious sedation in microlaparoscopy. J Am Assoc Gynecol Laparosc. 1997;4(5):591-594.
- Lent GS. Complex ear laceration. Medscape. May 10, 2018. Available at: https//emedicine.medscape.com/article/83294-overview. Accessed February 18, 2019.
- Lalonde D, Martin A. Epinephrine in local anesthesia in finger and hand surgery: the case for wide-awake anesthesia. J Am Acad Orthop Surg. 2013;21:443-447.
