Published on
Urgent message: New data reveal that urgent care compares favorably with other practice environments when it comes to select key quality indicators.
Developing methods to assess the quality of healthcare in any clinical area is a complicated affair. Many individuals have devoted large parts of their careers to quality measurement, and several national organizations such as The Joint Commission and the National Quality Forum—exist solely for the purposes of measuring and ensuring the quality of healthcare delivered to patients in the U.S.
In the urgent care arena, however, the field is less well developed. Very few measures that have been developed for ambulatory care apply to the urgent care setting, with its focus on episodic care, because historically such measures have focused on providing longitudinal care for a panel of patients. These include common measures such as those related to HgA1c testing for diabetic patients, the initiation and maintenance of antidepressant use, and utilization and timeliness of preventive screening tests such as mammograms.
On the hospital side, most measures focus on either inpatient services (such as hand washing or postsurgical infection rates) or on care for a very narrow range of conditions (such as providing aspirin for patients with acute myocardial infarction).
Again, this makes such measures less applicable to urgent care centers. As part of a larger project to survey urgent care centers and provide benchmarking data, we asked centers to tell us about a variety of activities related to quality of care, including how they are integrated with the rest of the healthcare system, their use of clinical practice guidelines, and how they measure quality of care and patient satisfaction.
What We Did
As noted in the January issue of JUCM, we identified urgent care centers for our benchmarking initiative using three methods.
First, we searched the website of each state’s health insurance commissioner, as well as websites sponsored by insurers’ trade associations to identify all health insurance carriers doing business in every state.
Each insurance carrier’s website was searched to locate all urgent care centers that are identified as having contracts or referral arrangements with that carrier.
Second, we searched www.yellowpages.com, www.super pages.com, and www.switchboard.com using a variety of terms such as “urgent care” and “walk-in clinic,” retaining only relevant listings. Third, we used the UCA and JUCM mailing lists. Duplicates that emerged from these three methods were counted only once.
Next, we selected urgent care centers at random from within four geographic areas of the U.S. (Northeast, Midwest, South, and West). Selected centers were invited to participate in a mail survey; those that did not respond were contacted multiple times by telephone.
The survey, which was conducted between January and March 2008, included questions on a wide range of topics, such as services provided, hours of operation, connections to other sectors of the healthcare system, use of health information technology, staffing, and financial data.
Prior to completing the survey, all organizations were screened to ensure that they were urgent care centers. To qualify, an urgent care center was required to:
- provide care primarily on a walk-in basis
- be open every evening Monday through Friday
- be open at least one day over the weekend
- provide suturing for minor lacerations, and
- provide onsite x-rays
This definition has been used in previous work, and was developed in conjunction with the UCABenchmarking Committee.1
Our final results are based on responses from 436 urgent care centers. The survey response rate, calculated using Response Rate 3 from the American Association for Public Opinion Research Standard Definitions, was 50.2%.2
What We Learned
Table 1 shows information on how urgent care centers are integrated with the rest of the healthcare system.

Overall, 55% of centers have at least one physician with admitting privileges at a local hospital. By comparison, 77% of practicing family physicians have admitting privileges.3 This difference is to be expected, however, since urgent care centers typically do not follow their patients over time or if they are hospitalized.
Referring
Many centers maintain lists of primary care (86%) and specialty (95%) physicians to whom they can refer patients. However, approximately 14% of centers do not have such lists of primary care physicians.
Maintaining lists such as these can be beneficial for those centers looking to build relationships with other practices in their community.
In addition, continuity of care is one key component of healthcare quality, as it can affect the efficiency with which services are delivered (eliminating duplication) and the patient-centeredness of the care provided. Maintaining such lists can help urgent care centers increase continuity of care for their patients.
Post-visit follow-up
Urgent care centers take a variety of actions after seeing a patient, including not contacting the patient’s regular physician, sending a copy of the chart or a consult note to the regular physician, or calling the regular physician. The action selected for any individual patient may depend on a variety of factors, such as whether the patient has a regular physician, how acute and/or serious the patient’s condition is, and the urgent care center’s policies and practices.
Again, since continuity of care is one significant aspect of healthcare quality, providing follow-up information to patients’ regular physicians can be a key component of high-quality urgent care. Board-certified physicians
Approximately three quarters of physicians working in urgent care are board certified (see Figure 1), which compares well against the 71% of primary care physicians who are board certified.4
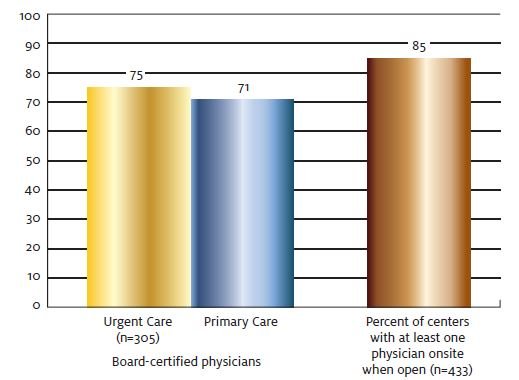
Eighty-five percent of centers have at least one physician on staff whenever the site is open.
Figure 2 illustrates the use of clinical practice guidelines in urgent care centers. For both general treatment decisions and specifically for antibiotic prescribing, slightly less than half of urgent care centers report using clinical practice guidelines “often.” While there are no benchmarking data available regarding how often primary care physicians refer to such guidelines, previous research has shown that patients typically receive only about half of the care that is recommended, with little difference in compliance with recommendations for acute care, chronic condition care, and preventive services.5

Quality of care
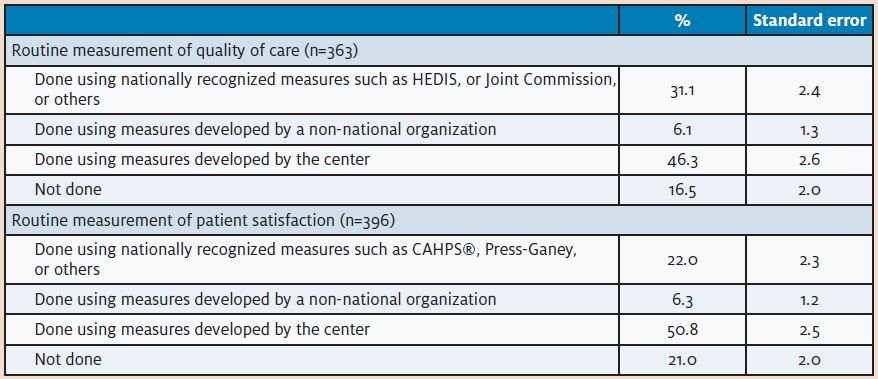
Finally, we asked how urgent care centers measure quality (Table 2).
Approximately 30% of urgent care centers routinely measure quality of care using nationally recognized measures such as the National Committee for Quality Assurance’s Healthcare Effectiveness ata and Information
Set (HEDIS), measures from The Joint Commission, or others.
By comparison, 20% of all physicians nationally report receiving quality of care data about the proportion of their patients who receive recommended care, and 18% receive data on patients’ clinical outcomes (such as glycemic control for diabetic patients).6
However, 46% of urgent care centers assess quality using measures they have developed themselves, and 16.5% do not measure the quality of the care they provide. Patient satisfaction Twenty-two percent of urgent care centers routinely assess patient satisfaction using nationally recognized tools such as CAHPS®, Press-Ganey, or other satisfaction surveys. By comparison, 25% f all physicians nationally report receiving data from patient surveys on experiences with care.6
Just over half of all centers report assessing patient satisfaction using measures they developed themselves. This may include assessing patient complaints or referrals, or using other methods for understanding how satisfied patients are. However, if centers are developing their own questionnaires to measure satisfaction, these measures may not have been validated using established survey methods.
One out of five urgent care centers does not assess patient satisfaction at all, which may represent a missed opportunity to understand patient perception of their services.
Measuring Quality
Measuring the quality of healthcare in the U.S. is essential to ensuring that such services make an optimal contribution to improving Americans’ health. The Institute of Medicine has defined six components of high-quality healthcare:
- safety
- timeliness
- effectiveness
- efficiency
- patient-centeredness
- equality.7
Without assessing each of these dimensions on a periodic basis, it is impossible to understand the state of the quality of care provided at urgent care centers, and where there may be opportunities for improvement.
At the same time, not all measures are created equal, and careful thought needs to be given to developing and selecting appropriate measures.
Someone who is not a clinician but has had a few infections may have some knowledge of antibiotics, but it is still preferable to have someone with clinical training and experience decide whether an antibiotic is necessary and which one is most appropriate. Similarly, individuals and organizations with expertise in quality measurement can help urgent care centers develop appropriate easures and survey tools, and can help to effectively tell the story of the quality of care provided at urgent care centers and the role they play in the larger healthcare system.
References
1. Weinick RM, Betancourt RM. No appointment needed: The resurgence of urgent care centers in the United States. 2007. California HealthCare Foundation. Avilable at: www.chcf.org/documents/policy/NoAppointmentNecessaryUrgentCareCenters.pdf.
2. The American Association for Public Opinion Research. Standard Definitions: FinalDispositions of Case Codes and Outcome Rates for Surveys. Revised 2008. Available at:
www.aapor.org/uploads/Standard_Definitions_07_08_Final.pdf.
3. Facts About Family Medicine. Table 31: Hospital admission privileges of family physicians by census division, July 2008. American Academy of Family Physicians. Available at: www.aafp.org/online/en/home/aboutus/specialty/facts/31.html.
4. Smart DR. Physician Characteristics and Distribution in the U.S.: 2006 Edition. AMA Bookstore.
5. McGlynn EA, Asch SM, Adams J, et al. The quality of health care delivered to adults in the United States. N Engl J Med. 2003;348(26):2635-2645.
6. Audet AM, Doty MM, Shamasdin J, et al. Measure, learn, and improve: Physicians’ involvement in quality improvement. Health Aff. 2005;24(3):843-853.
7. Institute of Medicine Committee on Quality of Health Care in America. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academy Press, 2001.