Published on
Mr. J.V. is a 28-year-old white male who presented to urgent are with a six-hour history of chest pain described as pressure in the sternal area radiating to the left shoulder; back pain was a 5/10 at time of visit, and constant with no accompanying nausea, dizziness, vomiting, or diaphoresis.
The patient described an inability to breathe deeply and a sensation of water stuck in the mid esophagus when drinking. Of note, he had similar episodes which resolved.
Observations and Findings
Well-appearing male in no distress.
Pmhx: childhood asthma
Meds: Allegra prn
Social hx: no drugs, etoh, or tobacco
Ros: no recent illness, no abd pain, no lbp, no extremity pain, no headache, syncope, no confusion, no cocaine use
Physical: t-96.7, p89, rr14, bp110/80, o2 sat 97% ra, peak flow 500
HEENT: nl neck: no jvd, no retractions
Resp: ctab no wheezes, no crackles
Cor: rrr no m/r/g
Gi: +bs ntnd, no rbnd or grdng, no pulsatile masses
Musculoskeletal: pain on palp along chest wall parasternal but no crepitations
Diagnostic testing: EKG which revealed sinus arrhythmia and incomplete rbbb
Diagnosis
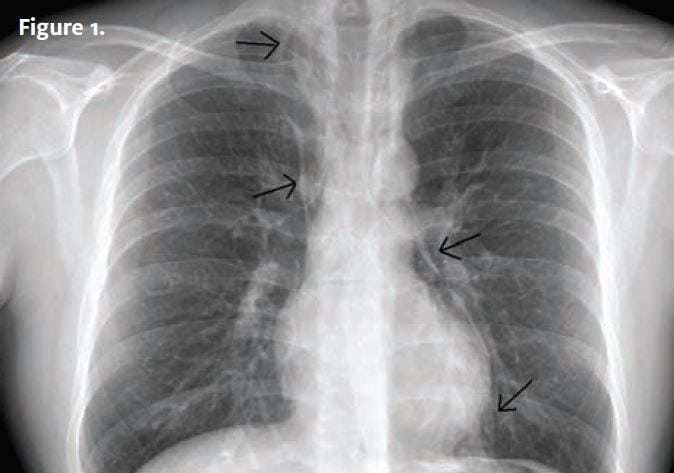
The x-ray reveals extensive pneumomediastinum with air surrounding the heart and anterior aorta and extending into the superior mediastinum and lower neck (Figure 1).
Discussion
Pneumomediastinum or mediastinal emphysema is a condition in which air is present in the mediastinum. This can be caused by trauma or disease. It is uncommon and occurs when air leaks from the lung or airways into the mediastinum.
Causes: Excessive coughing, sneezing, vomiting, or repeated valsalva maneuvers such as during childbirth or defecation. It may also occur during rapid ascents in altitude or scuba diving. It can also be associated with pneumothorax or other diseases (e.g., COPD or asthma).
Symptoms: Usually, chest pain below sternum that may radiate to neck and arms. Pain may be worse with breathing or swallowing.
Signs and tests: On physical, crepitations may be felt. Chest x-ray confirms presence of the abnormality.
Treatment
Often, no treatment is required as air is absorbed from the mediastinum. If pneumothorax is present, a chest tube is required. In rare cases, large amounts of air may compress veins affecting blood pressures.
Course of illness: In our patient, furthur investigation revealed no precipitating cause for the abnormality.
Follow up x-rays revealed reabsorption; the patient returned to normal activity without complaints.
Case submitted by Michael Talkar, MD, family/urgent care physician, locum tenens currently on assignment in Arizona.
