Published on
Urgent message: While pediatric elbow injuries can be a simple fix in an urgent care setting, understanding mechanism of injury and recognizing cases where referral is warranted help ensure positive outcomes.
Pediatric musculoskeletal injuries comprise approximately 12% of the 10 million annual visits to urgent care centers and emergency departments in the United States. History, physical exam and proper imaging remain the mainstay of diagnosis and treatment of many orthopedic related chief complaints. The purpose of this article is to provide a simple and concise approach to evaluation of common pediatric elbow pathology in the setting of a recent elbow injury.
Radial Head Subluxation
Case Presentation
Radial head subluxations are the most common cause of arm disuse in children and is a unique elbow injury in children <5 years of age. With sudden traction on the distal radius, a portion of the annular ligament slips over the head of the radius and slides into the radio-humeral joint where it becomes trapped.2
History
This often occurs as the caregiver grabs the arm to prevent the child from falling or pulling away, or when a child is swung by the forearms during play. Radial head subluxations also occur during sleep if the forearm is rolled over. The child will hold the arm close to the body with the elbow either fully extended or flexed and pronated. There is tenderness over the anterolateral aspect of the radial head and pain with supination of the forearm.3
Making the Diagnosis
The diagnosis is made clinically with history and physical exam. Imaging should only be obtained
to exclude a fracture or dislocation when history indicates an injury other than a minor pull or twist, or exam demonstrates focal tenderness or edema. On plain films, the radial head should point toward the capitellum in all views.1 A Monteggia fracture is a dislocated proximal radial-ulnar joint associated with a forearm fracture.
Management
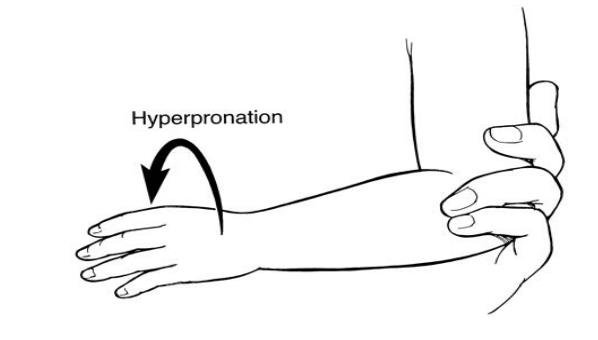
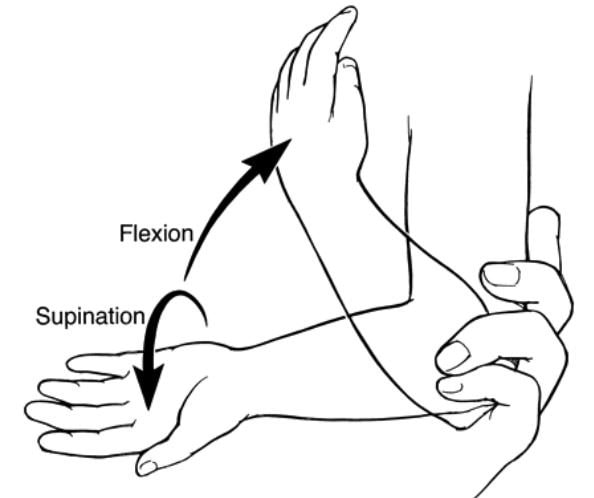
Two techniques utilized for reduction include supination/flexion and hyperpronation methods. Following successful reduction, there is immediate pain relief. Reduction is confirmed when the child moves the affected arm, which typically occurs within minutes. After successful reduction, no additional treatment, immobilization, or activity restriction is necessary.
Supracondylar Fractures
History
Supracondylar fractures account for 60% of pediatric elbow fractures and are usually caused by a fall on an outstretched hand. Careful examination is needed because there is significant potential for neurovascular compromise.1 Elbow effusions, decreased motion, and pain are common.
Making the Diagnosis
Examination should include evaluation for median, radial, or ulnar nerve injury. The median nerve is the most commonly injured nerve in supracondylar fractures. Median nerve injury will result in a weak “OK” sign or lack of distal interphalangeal flexion when making an “OK” sign.2 Injury to the radial nerve results in weakness of wrist extension, hand supination, and thumb extension (“thumbs up” sign). In addition, altered sensation is found in the dorsal web space between the thumb and index finger. Ulnar nerve injury causes weakness of wrist flexion and adduction, finger spread, and flexion of the distal phalanx of the fifth digit. This can be tested by asking the patient to firmly hold a piece of paper between the third and fourth digits.2
An indirect indicator of hemorrhage or effusion is displacement of the posterior fat pad, known as a “sail” sign, and indicates an occult fracture.4 On a normal elbow x-ray, the anterior humeral line runs through the anterior cortex of the humerus and intersects the capitellum in its middle third. There are three types of supracondylar fractures:5
Type I – Nondisplaced. Has an anterior humeral line that intersects the capitellum, an intact olecranon fossa, no medial or lateral displacement, no medial column collapse, and a normal Baumann angle.
Type II – Extends but does not completely transect with some cortical contact. Anterior humeral line does not intersect the capitellum.
Type III – Has a circumferential break in the cortex with displacement of fracture fragments.
Management
Disposition depends on whether the fracture is stable or unstable. Stable closed fractures can be discharged home in a posterior arm splint with orthopedic follow up within one week. Patients with open fractures need to be transferred to a facility with pediatric orthopedics on staff who can immediately reduce these fractures, a lack of immediate intervention can lead to permanent nerve damage and/or.6
Salter-Harris Fractures
Salter-Harris fractures are physeal fractures that are classified as type I, II, III, IV, or V. A common way to remember the fracture line and its relationship to the growth plate is:
S – Straight across (type I)
A – Above (type II)
L – beLow (type III)
T – Through (type IV)
ER – ERasure of growth plate (type V)
These fractures are best seen on AP and lateral views on the bones. Type I fractures are difficult to see on a plain x-ray, but bony tenderness on palpation aids in diagnosis. Nondisplaced type I and II fractures of the elbow can be immobilized with a short-arm splint and placed in a sling for 3 weeks.1 Volar splinting is preferred for type I, and sugar tong splinting is generally used for type II fractures. For displaced type I and II fractures, the extremity should be splinted and placed in a sling with urgent orthopedic consult for fracture reduction within the first 7 days. If type III, IV, and V fractures are identified in the urgent care setting, pediatric orthopedic evaluation is needed for reduction and possible internal fixation.7
A buckle fracture occurs at the distal metaphysis, where the bone is most porous, usually in younger children. This injury is caused by buckling of the cortex due to compression failure. Torus fractures are stable, and treatment is aimed at pain relief, comfort, and protection of the bone from any further injury using a short-arm cast or a splint.8
Children with splints may remove them at home after 3 weeks without orthopedic follow-up, but the patient should follow up with the primary care provider in 10-14 days. Orthopedic evaluation should occur for children with torus fractures and bowing of the arm, diminished range of motion, and continued pain. However, most children with buckle fractures do not require orthopedic follow-up.7
Olecranon Fractures
Olecranon fractures may occur when the child falls directly onto a flexed or extended elbow, or with a fall on outstretched hand with valgus stress on the forearm. The child usually presents with pain, tenderness, and/or edema to the olecranon region. Associated fractures are commonly greenstick or metaphyseal stress fractures. Challenges to identifying olecranon fractures include the inability to visualize the fracture on an AP view, the fact that the ossification center is an epiphysis and may normally appear separated or irregular, and multiple ossification centers on the lateral view may be misinterpreted as fractures. Contralateral elbow plain films may be obtained for comparison. Greenstick or stress fractures with minimal to no displacement may be treated with a cast, with about 20⁰ of elbow flexion; this reduces the distracting pull of the triceps muscle and allows proper healing. Follow-up consists of weekly x-rays for 2-3 weeks. Fractures with a step off >2 mm, displacement, or comminution with associated radial head or neck fractures require surgical intervention.1
Coronoid Fractures
Coronoid fractures occur from a fall on an outstretched hand or direct fall on the elbow. Symptoms consist of pain, tenderness, and decreased range of motion. Type I involves the tip of the coronoid process; type II involves <50% of the coronoid; and type III involves >50% of the coronoid.4 A “B” subset of each type indicates dislocation of the fragment. For nondisplaced fractures, patients can be placed in a long-arm posterior splint with the elbow in 90⁰ of flexion and the forearm in supination. Patient should have an orthopedic evaluation in 2 weeks. Displaced coronoid fractures should be transferred for emergent orthopedic evaluation for fragment fixation.
Septic Arthritis
History
Joint infection can be bacterial, fungal, or viral in etiology, but bacterial infection is the most common. Bacterial arthritis usually occurs in a single joint, most often of the lower extremity. Infections of the knee, hip, and ankle consistently account for at least 80% of cases, with the hip and knee affected most commonly.9 Bacterial arthritis presents classically with acute onset of fever and joint pain, swelling, limited range of motion, and possibly skin lesions. The extremity is held in a position of comfort.
Making the Diagnosis
Important questions to ask the patient and parents concern immunization status, recent penetrating joint trauma or injury, previous history of bacterial arthritis, recent surgery, recent illness, and insect bites.10 Obtaining a proper history will aid evaluation for traumatic joint effusion, ligamentous injuries, juvenile idiopathic arthritis, gout, Lyme disease, and avascular necrosis.
Management
When suspecting a septic joint, initial imaging consists of x-rays to rule out osteomyelitis, fractures, or inflammatory arthritis. An ultrasound can be obtained to examine for effusion. Important lab work to order includes complete blood count, blood cultures, and synovial fluid analysis (ie, WBC count and differential, gram stain, culture, susceptibility testing) if possible. The patient should be started on broad-spectrum IV antibiotics.9 The final disposition of the patient should be transfer to the closest hospital with pediatric orthopedics for further evaluation and treatment.
Summary
Obtaining an accurate history from a pediatric patient can be difficult, possibly due to inability of the patient to verbalize or properly convey their feelings. Thus, an important aspect of an urgent care evaluation of a pediatric patient following an injury is a thorough physical exam and a low threshold for imaging. Commonly encountered injuries include supracondylar fractures, radial head subluxation, and Salter-Harris fractures, but septic arthritis, coronoid fractures, and olecranon fractures should also be considered. If the history or evaluation is suspicious for a complicated elbow injury, immediate referral or transfer from the urgent care center should take place.
Tulja Parmar, DO; Alicia Roman-Colon, MD; Christopher Tangen, DO
Citation: Parmar T, Roman-Colon A, Tangen C. Pediatric elbow assessment: an urgent care approach. J Urgent Care Med. March 2017. Available at: https://www.jucm.com/pediatric-elbow-assessment-urgent-care-approach/.
References
- Shrader MW. Pediatric supracondylar fractures and pediatric physeal elbow fractures. Orthop Clin North Am. 2008;39(2):163-171.
- Young GM. Reduction of common joint dislocations and subluxations. In: Henretig FM, King C, eds. Textbook of Pediatric Emergency Procedures. Baltimore, MD: Williams & Wilkins; 1997.
- Koelink E, Schuh S, Howard A, et al. Primary care physician follow-up of distal radius buckle fractures. Pediatrics. 2016;137(1). Epub 2015 Dec 10.
- Carson S, Woolridge DP, Colletti J, Kilgore K. Pediatric upper extremity injuries. Pediatr Clin North Am. 2006;53(1):41-67.
- Herring JA. Tachdjan’s Pediatric Orthopaedics from the Texas Scottish Rite Hospital for Children. 4th ed. Philadelphia, PA: Saunders Elsevier; 2008.
- Joffe M, Loiselle J. Musculoskeletal emergencies. In: Shaw KN, Bachur RG, eds. Fleisher and Ludwig’s Textbook of Pediatric Emergency Medicine. 7th ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2015:1390.
- Chadwick CJ, Bentley G. The classification and prognosis of epiphyseal injuries. Injury. 1987;18(3):157-168.
- Baratz M, Micucci C, Sangimino M. Pediatric supracondylar humerus fractures. Hand Clin. 2006;22(1):69-75.
- Krogstad P. Septic arthritis. In: Cherry JD, Harrison GJ, Kaplan SL, et al, eds. Feigin and Cherry’s Textbook of Pediatric Infectious Diseases. 7th ed. Philadelphia, PA: Elsevier Saunders; 2014:727.
- Nade S. Septic arthritis. Best Pract Res Clin Rheumatol. 2003;17(2):183-200.