Published on
 Differential Diagnoses
Differential Diagnoses
- Osteoarthritis
- Mallet finger
- Gamekeeper’s thumb
- Rheumatoid arthritis
- Osteosarcoma
Physical Examination
The patient is afebrile, he has a pulse rate of 120 beats/min, his respiration rate is 20 breaths/min, and his blood pressure is 110/89 mm Hg. He is and oriented, is not in acute distress, but is holding his right hand in his lap. There is swelling of the hand, and he experiences a moderate amount of pain with palpation over the metacarpophalangeal (MCP) joint of the little finger. He has pain with even a minimal range of motion. He has no tenderness over the proximal interphalangeal or distal interphalangeal joints of the little finger or over the MCP of the ring finger. His wrist is not tender with palpation, and it has good range of motion. The neurovascular status is intact, with a 2+ radial pulse, and sensation is grossly intact.
Diagnosis
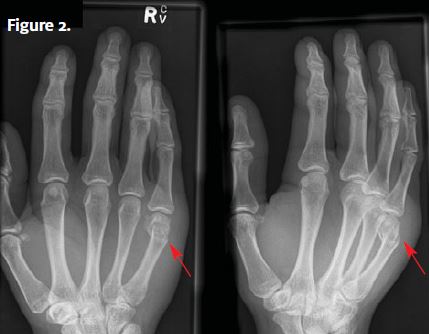
A hand x-ray (Figure 2) is obtained that confirms a fracture of the distal metacarpal bone of the little finger with 30° of angulation. The patient has a boxer’s fracture.
Learnings
A boxer’s fracture is a distal metacarpal fracture of the middle, ring, or long finger. It is one of the most common hand injuries occurring in young males who strike an object such as a wall or a face with a closed fist.
There are five metacarpal bones in the hand, with the proximal aspects meeting the eight bones of the wrist and the distal aspects meeting the phalangeal bones of each finger. The index, middle, ring, and little fingers each have three phalanx bones: the proximal, middle, and distal phalanx bones. The thumb has two phalanx bones, the proximal and the distal.
The mechanism is typically a blunt force against the MCP of the little finger. Note that a very vigorous mechanism may result in a carpometacarpal dislocation or an open fracture. A fracture resulting from a fight where the hand comes in contact with a mouth can result in oral organisms causing a skin or bone infection. These injuries are called closed-fist injuries, or fight bites. Patients may be reluctant to reveal the etiology of the injury for fear of legal or other issues. Injuries often present with a laceration over the MCP joint of the middle, ring, or little finger.
What to Look For
The physical examination should include the following:
- Inspection of the skin for swelling, abrasions, and lacerations
- Palpation of the area of greatest pain as well as the joint proximal and distal to the injury
- Assessment of strength; strength may be preserved with up to 90% disruption of a tendon
- Assessment of neurovascular status; document sensation and pulse or capillary refill
By using a stepwise approach to evaluation of a hand x-ray, the clinician can avoid missing important findings. Start with the metacarpal bones, looking for alignment, signs of soft-tissue swelling (indicating location of greatest injury), and fracture. Watch for
- A break in the cortex on any of the three x-ray views
- Disruption in trabeculations
- Lucency within the bone
- Angulation or impaction
Next, evaluate the bones of the wrist (carpal bones) for fracture or dislocation. Obtain a dedicated wrist x-ray if there is any wrist pain with palpation or range of motion.
Should a boxer’s fracture be reduced, or should it be splinted? If there is angulation of <40° of the fracture, this will not result in loss of function and does not require reduction. The patient should be cautioned that there may be a cosmetic deformity. Provide ice, immobilization with an ulnar gutter or volar splint, elevation, and a referral to an orthopedist or hand surgeon within 2 or 3 days.
The following are indications for transfer to an emergency department:
- Open fracture
- Carpometacarpal dislocation
- Open wound with infection
- Osteomyelitis
- Intractable pain