Published on
Urgent message: With patients who have sustained head injuries related to both sports- and non–sports-related activities presenting to urgent care more than ever before, it’s essential for the provider to have a nuanced understanding of which patients truly require transfer or referral to a high-acuity level of care, and which can be managed successfully and safely in the urgent care setting.
Anthony P. Doran, PsyD; Robert G. Graw, Jr., MD; Marc Weber, MD; Stanford Coleman, MD; Kevin Crutchfield, MD; and Daniel Pokrifka, ATC
ABSTRACT
Background
Urgent care, family practice, and pediatric clinicians and researchers have debated for years whether patients with a mild traumatic brain injury (mTBI) need immediate imaging after injury. HeadFirst is a community-based concussion clinic with locations throughout Maryland that evaluates an average of 1,300 mTBI patients per month. We reviewed data from patients who were diagnosed and treated from January 2016 through December 2018.
Objective
A constant question among primary care physicians and in urgent care centers is whether all patients seen with a head injury require CT or MRI imaging to assess for intracranial bleeding.
Methods
Researchers examined transfers of patients with a diagnosis of mTBI from 18 community-based urgent care centers to local emergency departments between January 2016 and December 2018. A total of 17,451 consecutive urgent care patients with head injuries and mTBI, were reviewed for evaluation, diagnosis, need for emergent neuroimaging and results of neuroimaging, using multiple validated assessment techniques.
Results
Of the 17,451 patients reviewed, 843 (4.8%) were transferred to the emergency department for imaging; only four (.02%) evidenced positive results on CT scan. Results suggest that urgent care clinicians can rely on their clinical evaluation in making decisions regarding need for higher level of care or brain imaging. A solid mTBI examination that includes a thorough history, neurological and physical exam, subcortical evaluation (examination of ocular, nerve and balance functioning), and neurocognitive testing can assist the clinician in making decisions about patient care.
INTRODUCTION
Traumatic brain injuries account for between 6% and 9% of all athlete injuries among United States high school and college athletes.1 An mTBI is a blow to the head or body that causes axonal and rotational forces to the brain that can be observed by self-report of physical, cognitive, emotional, and sleep symptoms; subtle changes to cranial nerves; alterations in ocular-motor and balance functioning; or a change in neurocognitive functioning. Self-reported symptoms and changes in functioning from an mTBI can last days, weeks, months and in some cases much longer. With over 1.7 million people in the U.S. seeking medical attention for head injury each year, clinicians are challenged to identify the small subgroup of patients who possibly have sustained a potentially lethal intracranial bleed while minimizing radiation exposure and unnecessary cost from diagnostic testing and hospital admissions.2 Researchers estimate there are over a million mTBI-related ED visits in the U.S. annually. Children aged 0–14 years were more likely to be seen in the ED; typically, males outnumber females 3 to 1.3 Children (under 14) and the elderly (over 85) were the most frequently seen in the ED for mTBI.4,5 The most common mechanisms of injury were falls, motor vehicle accidents (MVAs) and being struck by an object; only 20% were sports-related.
Several studies have examined the presence of mTBI in the ED. Researchers examined data from U.S. hospitals that provide emergency services in the National Electronic Injury Surveillance System (1997–2007) and All Injury Program (2001–2005).6
Half of all ED visits involving concussion were sports-related, with 14–19 year-olds making up 60% of these visits. Of the sports-related injuries, only 25% were sustained during organized team sports (OTS). From 1997 to 2007, although participation in OTS during the study period declined, ED visits for concussions related to OTS in 8–13 year-old children doubled.6
Other researchers surveyed a sample of 522 athletes and found that 20% reported concussion-like symptoms after being hit in the head the previous year, yet 89% of patients did not recognize that they had a concussion. Headache was the most common symptom of mTBI.7 Confusion/disorientation was second in recognized mTBI and dizziness was second in unrecognized mTBI. Nausea was the most common reason for someone to seek medical attention, followed by loss of consciousness and memory problems.7
Some scientists measured the number of pediatric patients with concussions in EDs and the treatment they received. Data collected from children’s hospitals in the Pediatric Health Information System show that ED visits for concussion more than doubled from 2001 to 2010 (2,126 vs 4,967; <.001),8 while total admissions remained the same. Further, 60% of ED visits for concussion received a computed tomography (CT) scan and about 47.7% received medication (most frequently: non-narcotic painkillers) or IV fluids.8
Although a number of studies have examined primarily the epidemiology and incidence rates of mTBI in the ED, few have examined the efficacy of a clinician’s tools utilized in the examination of a patient’s head trauma in making the determination whether the patient should receive imaging.
Righttime Medical Care is an urgent care facility with 18 locations in Maryland. HeadFirst is a community-based concussion clinic located within 12 of the Righttime Care Centers. The two provide a community-based continuum of care for mTBI. Righttime Medical Care began evaluating patients with head injury in 2011. A retrospective review was conducted to assess if clinicians (physicians, nurse practitioners, physician assistants, and neuropsychologists) in an outpatient urgent care facility could accurately and reliably predict (utilizing standard history and physical assessment skill) the need for radiological imaging in patients with suspected mTBI.
METHODOLOGY
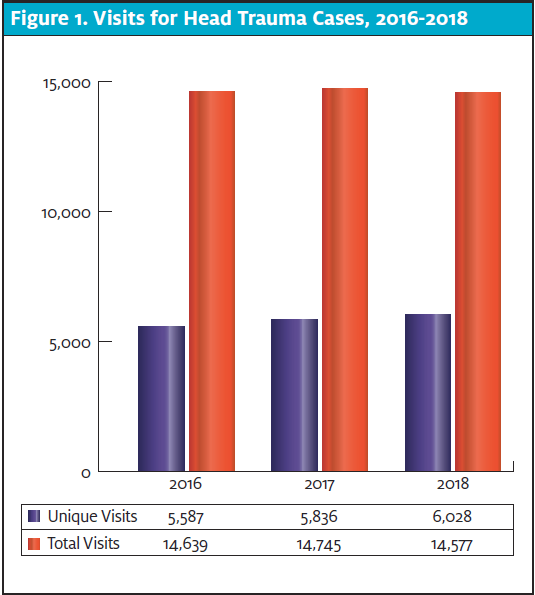
In this study, researchers examined emergency department transfers from 18 community-based urgent care clinics with a diagnosis of mTBI to surrounding area EDs from January 2016 to December 2018. During that span, 17,451 unique head trauma cases were seen at these urgent care clinics (Figure 1).
Clinicians used the Acute Concussion Evaluation (ACE)9 to gather history and information about the patient’s head trauma, present symptoms, comorbid diagnoses, and risk factors.
After performing a complete and thorough standard physical and neurological examination, clinicians further assessed cranial nerves, balance, and ocular-motor functioning. This assessment included consideration of the Canadian CT Head Rule (GCS score <15 at 2 hours after injury; suspected open or depressed skull fracture; any signs of basal skull fracture; vomiting >2 episodes; age >65; amnesia before impact >30 mins; dangerous MOI; Pediatric – GCS score <15 at 2 hours after injury; suspected open or depressed skull fracture; any signs of basal skull fracture; vomiting >2 episodes; dramatically worsening headache or irritability; large hematoma (>5cm) on the scalp; dangerous MOI).10 Following the initial assessment of each patient by the assigned medical provider, the findings were discussed with a HeadFirst Medical Director before the transfer to the ED. Each and every head trauma is maintained in an electric record and manual spreadsheet for ease of patient identification and program improvement.
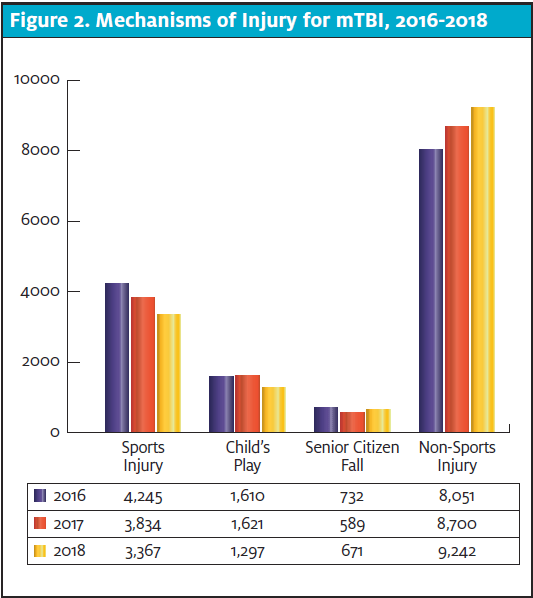
Per these sources of information, 843 patients were transferred to the ED. The ages of these ED transfer patients ranged from as young as 2 months to 96 years old. The average age was 40; 108 (12.8%) of the transfer patients were younger than 8 years of age; 353 (41.8%) were 9 to 64 years of age; and the remainder were 65 or older (n=382, 45.3%). Each gender was nearly equally represented with 453 (53.7%) females and 390 (46.2%) males. An examination of the breakdown of all mTBIs in our sample is in Figure 2.
RESULTS
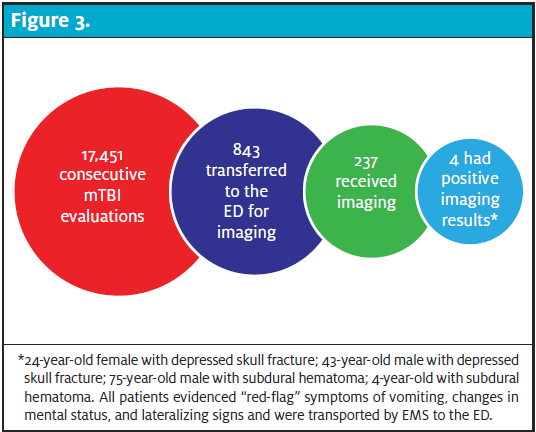
Of the available ED transfer patients, senior medical officer and clinic staff following up with head trauma patients (n=743), 247 (36%) reported being imaged in the ED; the remainder were monitored and released for outpatient follow-up. Of the patient’s that did receive imaging, two patients had a positive CT scan due to depressed fracture (24-year-old and 43-year-old) and two subdural hematomas (one 75-year-old and a 4-year-old). These patients had abnormal findings on neurological and cranial nerve examinations and clinicians knew that neuroimaging would be positive (Figure 3).
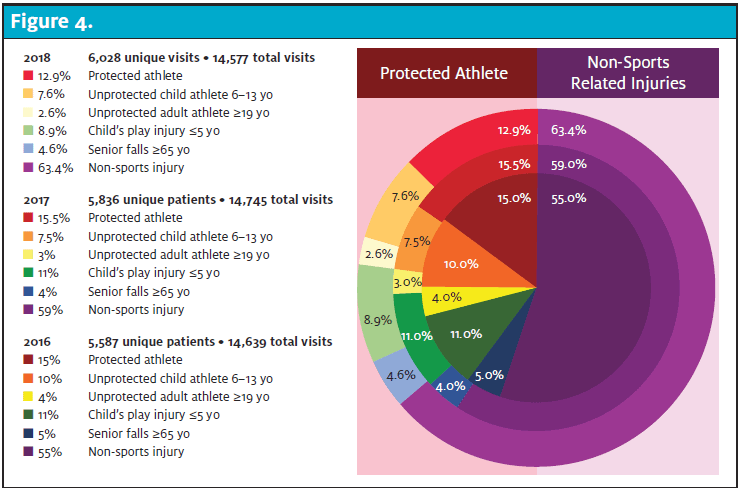
Out of 843, 750 (89%) were non–sports-related and only 93 (11%) were sports-related. Of the non–sports-related injuries, the majority were falls or accidental in nature (n=581, 69%), and MVAs (n=118, 14%). A complete breakdown of all mTBIs from 2016 to 2018 is contained in Figure 4.
LIMITATIONS
This program analysis has several limitations. This analysis is a retrospective observational study with a convenience sample. As that suggests, while data collection was relatively convenient this sample may not represent the general population. There was a fair amount of attrition in that 12% of patients who could not be reached by phone or e-mail, even with multiple attempts by multiple staff. All such patients were sent a letter including clinic recommendations regarding imaging and following up with a concussion specialists and the risks of not following up with a medical professional. In theory, there could been several patients with serious neurological complications but it is unlikely they would not have circled back to inform clinic staff or providers.
DISCUSSION
Although sports-related concussions are more publicized, the majority of mTBIs self-referred or taken to the local ED are due to MVAs, falls (non–sports-related), and assaults. As can be seen from Figure 4, the percentage of “protected athletes” (those in programs with coaches, athletic trainers, and the support network of their school) has decreased over the years. This could be reflective of rule changes in youth sports, modification of play taught by coaches, or more athletic trainers, pediatricians, and family practice physicians being comfortable due to increased training and education in managing non-complicated concussion. Over the course of almost 3 years, with more than 5,000 new head traumas presenting to an urgent care clinic on a yearly basis, the transfer rate to the ED was 4.8%. The incidence rates seen in our sample is consistent with CDC data and research from other studies.
Overall, the data suggest that the urgent care setting is a safe environment in which to assess mTBI. Urgent care clinicians can make appropriate and thorough evaluations and observe patient functioning while assessing the need for referral to the next level of care due to more serious associated injury (ie, for evaluation of skull fracture, subdural or intracranial hematoma).
This study suggests potential modification of the decision rules for outpatient facilities in obtaining costly neuroimaging studies may be warranted. Clinicians who are experienced in the thorough, rigorous assessment of traumatic brain injury can safely and accurately assess the need for further imaging and predict intracranial complication.
REFERENCES
- Bryan MA, Rowhani-Rahbar A, Comstock RD, et al Sports and recreation-related concussion in US youth. Pediatrics. 2016;138(1):e20154635.
- Haydel M. Management of mild traumatic brain injury in the emergency department. Emerg Med Pract. 2012;14(9):1-24.
- Colantonio A, Saverino C, Zagorski B, et al. Hospitalizations and emergency department visits for TBI in Ontario. Can J Neurol Sci.2010;37(6):783-790.
- Guerrero JL, Thurman DJ, Sniezek JE. Emergency department visits associated with traumatic brain injury: United States, 1995–1996. Brain Injury. 2000;14(2):181-186.
- Jager TE, Weiss, HB, Coben JH, Pepe PE. Traumatic brain injuries evaluated in U.S. emergency departments, 1992-1994. Acad Emerg Med. 2000;7(2):134-140.
- Bakhos LL, Lockhart GR, Myers R, Linakis JG. Emergency department visits for concussion in young child athletes. Pediatrics, 2010;126(3):e550-e556.
- Delaney JS, Abuzeyad F, Correa JA, Foxford R. Recognition and characteristics of concussions in the emergency department population. J Emerg Med. 2005;29(2):189-197.
- Colvin JD, Thurm C, Pate BM, et al. Diagnosis and acute management of patients with concussion at children’s hospitals. Arch Dis Child.2013;98(12):934-938.
- Gioia GA, Collins M, Isquith PK. Improving identification and diagnosis of mild traumatic brain injury with evidence: psychometric support for the acute concussion evaluation. J Head Trauma and Rehab. 2008;23(4):230-242.
- Easter JS, Haukoos JS, Meehan WP, et al. Will neuroimaging reveal a severe intracranial injury in this adult with minor head trauma? The rational clinical examination systematic review. JAMA. 2015;14(24):22-29.
Acknowledgements: The authors would like to acknowledge their support staff—welcome desk and nurses and interns who helped make our patients feel welcome and comfortable while being assessed by clinicians at Righttime Medical Care and HeadFirst Sports Injury and Concussion Care.
Author affiliations: Anthony P. Doran, PsyD, HeadFirst Sports Injury and Concussion Care, Crofton, MD. Robert G. Graw, Jr. MD, HeadFirst Sports Injury and Concussion Care, Crofton, MD. Marc Weber MD, HeadFirst Sports Injury and Concussion Care, Crofton, MD. Stanford Coleman MD, HeadFirst Sports Injury and Concussion Care, Crofton, MD. Kevin Crutchfield, MD LifeBridge Comprehensive Concussion Clinic, Baltimore, MD. Daniel Pokrifka ATC, HeadFirst Sports Injury and Concussion Care, Crofton, MD. The authors have no relevant financial relationships with any commercial interests.