Published on
Urgent message: While few data specific to the urgent care setting exist, applying the medical evidence gleaned from other acute care settings can enable the clinician to effect positive outcomes in patients presenting with symptoms indicative of minor TBI.
Joseph Toscano, MD
Head trauma is among the most important problems evaluated in acute-care medicine. Estimates from the Centers for Disease Control and Prevention indicate that each year in the Unites States, approximately 1.4 million individuals suffer traumatic brain injury (TBI). Of these, 1.1 million are evaluated and released from emergency departments, 235,000 are hospitalized, and 50,000 die.1
While the exact number of patients with TBI who are cared for in urgent care centers is unknown, anyone working in that setting can attest that these patients present regularly for evaluation; over a quarter of TBIs result from falls, 20% from motor vehicle crashes, 11% from assaults, and the remainder from other head contusions and impacts.
A study published in January 2007 indicated that 911 calls from urgent care clinics occurred for pa- tients with head injury more often than for patients with EKG changes, GI bleeding, dehydration, and several other causes.2
After rapidly recognizing and stabilizing any potentially life- or limb-threatening injuries, the chief diagnostic decision when evaluating these patients in the acute care setting involves the ordering of CT scanning of the head. As discussed in the previous article in this series (JUCM, March 2008), several clinical decision instruments can help clinicians choose whom to image, though none may significantly reduce the number of CT scans performed, compared with clinical judgment alone.
This article will focus on the urgent care clinic application of the existing medical evidence (of which there is little that is high-quality and patient-oriented, unfortunately) and other recommendations for the care of these patients, and discuss some of the basic elements of treating minor TBI, as well as injury prevention.
Patient Scenarios
It is a busy, full-moon Saturday at the urgent care clinic and your medical assistant informs you that the staff has just roomed three patients, all with some degree of head injury:
- Patient A is a 3-month-old baby girl who, her mother reports, rolled off her dressing table and fell three feet onto the carpeted The child did not lose consciousness, but slept for about two and a half hours. When she awoke, the mom noted some bruising and swelling of the child’s scalp and so brought her in. The child had a normal feeding since the fall, has not vomited, and is behaving normally. Your exam confirms a scalp hematoma but is otherwise normal. How would you approach this patient? Would it be any different if the scenario and exam were similar, but the child was 4-years-old and fell to the ground while jumping like a monkey on his bed?
- Patient B is a 22-year-old who presents to the urgent care clinic with a friend two days after being hit in the side of the head by another friend’s knee during a backyard football game. It’s unclear, but he may have briefly lost consciousness; unfortunately, he has some retrograde amnesia and so cannot remember what he’s been told was a spectacular touchdown mHe has a moderate generalized headache which has not changed since the incident, but has not vomited and otherwise feels well. His physical exam is normal, except for some scalp tenderness in the area of impact. Does he need imaging and further treatment? Would your decision-making be different if you were evaluating him within an hour after the injury?
- Patient C is a 68-year-old patient who comes to the urgent care center with his wife several hours after he tripped and fell at home, hitting his tem- ple on a He did not lose consciousness and feels entirely normal. His exam reveals only a small abrasion on his temple. Nonetheless, he is concerned because a friend of his with a similar injury ended up being a “vegetable.” What would you advise? Would you advise differ- ently if the situation were the same, except that he were taking warfarin or another “blood-thinner”? We will discuss rationale for management of these patients later in this article.
Urgent Care Evaluation
It is intuitive that urgent care clinics develop procedures based on their capabilities for the rapid assessment of the (thankfully, rare) high-risk patient who presents with a history or symptoms which are suspicious for a significant intracranial injury. Such patients include those with abnormal behavior, obvious or highly suspicious skull fracture, any focal neurological deficits, drug- or alcohol intoxication, or Glasgow Coma Score (GCS) less than 15.
Staff should be trained to identify and promptly bring these patients to the treatment area of the clinic and notify the clinician. The clinician should perform a rapid primary general assessment, including obtaining a description of mechanism of injury, the patient’s past medical history, a determination of GCS, and an HEENT, neck, and neurological examination.
Clinical staff should carefully immobilize the patient, obtain vital signs, and examine the patient for other injuries while preparations are made for ambu- lance transfer to the nearest emergency department that could care for such a patient.
Any necessary stabilizing care that is within the clinic’s capabilities should be provided, including helping maintain a patent airway, providing ventilation and oxygenation, ensuring adequate circulation, and stabilizing any other injuries. Obtaining IV access and providing pain control are other potentially beneficial interventions.
Some of these patients can be combative or uncooperative and their care can be very difficult. Being prepared with standard protocols for such situations is advisable.
Patients without such high risk features can be triaged and evaluated in the same manner as any other stable patient. Once the patient is in the treatment area, a more in-depth history should be obtained; traditionally, this includes establishing whether there was any duration of loss of consciousness, amnesia, post-traumatic seizure, headache, nausea, or vomiting, though the exact implication of any of these findings in isolation is uncertain.
Inquiring about other areas of bodily injury can direct subsequent physical examination.
For patients involved in falls or collisions, asking about possible syncope or lightheadedness prior to the incident may indicate the need for further evaluation. Important past medical history includes whether the patient has a known or possible coagulopathy or takes medications such as warfarin, clopidogrel, or aspirin.
Physical examination of a patient with head injury often begins with inspection of the face and head. Ecchymoses in the infraorbital location (raccoon’s sign) or over the mastoid process (Battle’s sign) can indicate basal skull fracture.
Any areas of head impact should be palpated for possible closed fractures. With fractures, the skull may feel irregular, unstable, or boggy due to associated bleeding into adjacent soft tissues. Examine children carefully particularly those 2 years of age and under for scalp hematomas, as these are associated with increased risk of intracranial injury.
If a scalp wound is present, the clinician should gently palpate the area searching for fracture, externally at first. Wounds thus examined and without suspicion of skull fracture can then be examined internally in standard fashion, with subsequent wound debridement, irrigation, and closure as indicated if no fracture is seen. If a skull fracture is present on internal exam, it should not be further manipulated, but rather dressed with a sterile dressing, held in place with minimal external pressure.
An EENT exam should focus on possible associated injuries in these areas, as well as examining for hemotympanum, another indirect sign of a basal skull fracture. Young children may be examined for retinal hemorrhages, reported to be pathognomonic for child abuse. Horizontal or rotatory nystagmus may indicate vestibular dysfunction as a result of concussion, while vertical nystagmus is specific for cerebellar injury.
Because head impact can result in cervical spine injury, closely examine the patient’s neck for possible trauma. Reliable, high-quality clinical decision rules 3-5 do exist to support decisions regarding the need for cervical spine radiographs. The thoracic and lumbar spines, extremities, and torso can be examined if the history and symptoms suggest the need.
There is no reported standard neurological exam; however, assessing orientation and memory, cranial nerves, motor and sensory systems, cerebellar function, and gait can be done relatively quickly and would represent a reasonably complete exam.
Initial Imaging Decisions and Treatment
Though clinical judgment should prevail, a proposed algorithm for evaluating and treating patients with head injury was described in the previous article (available at www.jucm.com). Clinicians may care for other injuries e.g., splinting of probable fractures and initial wound cleansing and dressing in those who require referral for CT scanning and/or extended observation if this does not significantly delay transfer. Those who do not require referral may receive definitive evaluation and care for other injuries based on clinic capabilities.
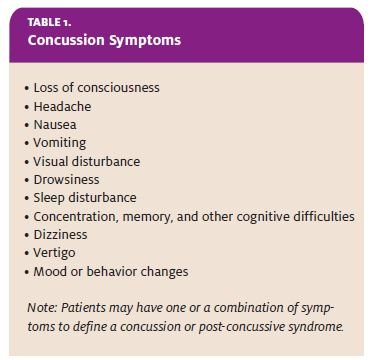
Patients cared for in the urgent care clinic after head injury may be asymptomatic or present with a variety of symptoms (Table 1). The term concussion or post-concussive syndrome is used to describe the common clinical sequelae of mild TBI. Symptoms can range from mild to severe; the specific neural insult in concussion, though not known for sure, probably relates to mild injury to the brain axons (more severe cases of diffuse axonal injury usually result in stupor or coma).
Concussive symptoms, in and of themselves, do not mandate CT scanning in the acute setting, though some type of imaging is typically performed if they persist or worsen. In situations where CT scanning is performed, the scan is usually normal in patients with concussion.
Many patients with concussion often desire relief from the associated symptoms. Initial management is typically directed toward the symptom itself—analgesics for headache, antiemetics for nausea, and meclizine for vertigo or dizziness can be considered.
There are no data to elucidate which are the best treatments, or even whether treatment is any better or worse than non-treatment, but most references recommend avoiding opiates, benzodiazepines, and other sedatives and hypnotics. Some of these have been shown to delay recovery in animal studies.
Because of the small risk of delayed intracranial bleeding, there may be at least a theoretical advantage of acetaminophen over nonsteroidal anti-inflammatory drugs to treat pain. Clinical judgment should prevail, and as always, basing treatment decisions on a mutual understanding of the individual risks and benefits for each patient is probably best.
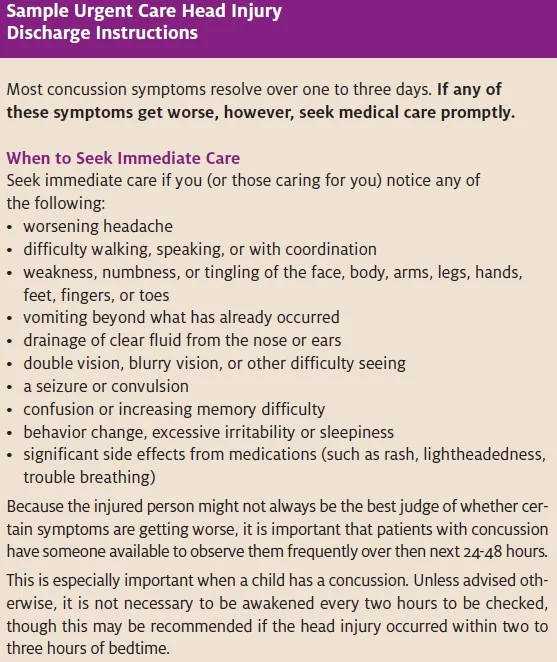
In addition to symptom management, ongoing observation is key in the management of any patient with head injury. The incidence and epidemiology of significant head injury becoming apparent on a delayed basis is not known, so all head injury patients should be given clear instructions regarding warning symptoms (such as the those suggested in the box on this page) and should have a reliable caregiver available, with ready access to follow-up medical care if needed.
The optimum period of observation is uncertain, but clinicians should convey the need for evaluation for any new or worsening symptoms in the hours to days after a head injury. Any patient with worsening level of consciousness or mental status, abnormal behavior, recurrent seizures, repeated vomiting, or the development of focal findings should be evaluated promptly, preferably in the emergency department, in conjunction with CT scanning of the head. An isolated but worsening headache after head trauma, though nonspecific, would also prompt imaging in most instances.
The decision rules described in the earlier article were derived and tested in patients within the first 24 hours after injury, and the value of their application beyond this time is uncertain. Typically, however, standard practice involves performing some type of neuroimaging for patients who develop worrisome symptoms on a delayed basis or for those who have ongoing symptoms and did not initially undergo CT scanning. The pathophysiological rationale for this relates to the possibilities of slow or delayed hemorrhage or edema development.
In patients with initially normal imaging results and no worsening or new symptoms, there is no need for repeat imaging after an initial nor- mal scan has been obtained. When the imaging findings are normal or do not require intervention, ongoing symptom management is of- ten the patient’s chief concern. In the majority of cases, symptoms decrease progressively over time; however, some degree of discomfort or cognitive or emotional difficulty may persist, in some patients for up to a year or more. Unfortunately, there is little evidence to inform the best approach for these patients, and many factors—e.g., underlying identifiable or occult brain in- jury, the patient’s general health and coping abilities, psychosocial stressors can combine to lead to ongoing symptoms.
A multidisciplinary approach is often required.
Treatment options at the urgent care level include low-dose tricyclic agents and selective serotonin reuptake inhibitors, which can help relieve many post-concussive symptoms. For patients with specific vestibular symptoms after concussion, vestibular rehabilitation with a physical therapist trained in these techniques can be helpful.
Patients with refractory or complicated symptoms require referral to a neurologist. Often, electroen cephalography or specialized neurocognitive testing is helpful. Requesting ophthalmology consultation for ongoing visual complaints is also prudent.
Return to Activities
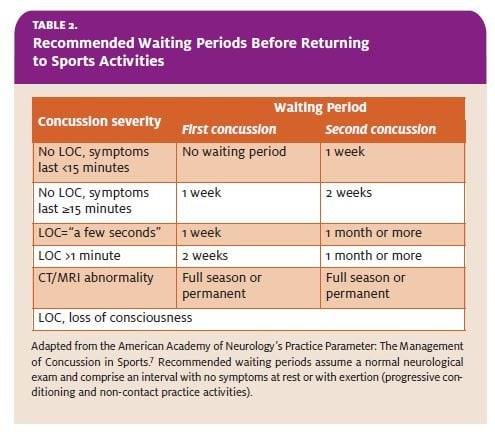
In general, patients may return to most activities on an “as tolerated” basis after head injury. This excludes, however, sports and other activities where there is a potential for repeated head injury. Several groups have published guidelines, based on consensus opinion, regarding when an athlete may re- turn to play, based on the severity and repetitiveness of injury.6,7 Having the athlete, once asymptomatic, return to light conditioning activities, where there is no potential for head injury, can help assess fitness for return to practice and play. In each case, the recommended delays assume that the athlete is asymptomatic at rest and with exertion for the prescribed interval, prior to return to sports (Table 2).
Recommendations for evaluating athletes on the field after head injury involve more complex determinations. Physicians in this role should become familiar with the recommended “sideline” neurological and physical examination and controversies prior to returning athletes to play on the same day.
Whether on the field or off, clinicians should emphasize the importance of proper equipment wear, fit, and usage to help decrease the impact of recurrent injuries. Returning to work after a head injury can be a more complicated process. The American College of Occupational and Environmental Medicine practice guidelines, unfortunately, include no mention of the subject so clinicians must use their judgment based on the severity of the injury, nature of any ongoing symptoms, and the patient’s specific job demands.
A supervised return to work-related tasks, with gradually and progressively increasing physical and mental demands, should be guided by regular re- assessment to determine how the employee is tolerating such advancement. Any persistent subjective complaints can be further evaluated with specific neurocognitive and other objective testing, to assist with ongoing case management and any necessary disability determinations.
Prevention
Clinicians should reinforce principals of proper helmet and protective equipment wear whenever possible, but particularly when a patient is being seen for a head injury. Reviews of various studies demonstrate that wearing a he met during bike riding or motorcycle riding significantly reduces the chance and severity of head injury.8,9 It is reasonable to conclude that this may also be the case with roller skating and skateboarding.
Return to Patient Scenarios
Patient A
Based on the presence of a scalp hematoma alone, this infant should be referred for CT scanning. Final disposition would then be based on the results of the scan. Head trauma can be a presenting injury in children who are victims of abuse; hence, when the mechanism of injury is uncertain or difficult to believe, additional screening for child abuse is warranted.
Because 3-month-olds are not physically capable of rolling, asking for some clarification of the history is important in this case. If the patient were a 4-year-old with a reasonable history of injury and a scalp hematoma as the only abnormality, discharge with recommendations regarding standard observation and follow-up (and maybe some admonishment regarding, “No more monkeys jumping on the bed!”) would be reasonable.
Patient B
If this patient had presented within 24 hours of injury, there would be no specific indication for CT imaging, except perhaps for his amnesia, though this would be a “judgment call.” With the history of two days of constant moderate symptoms, many clinicians would consider, for risk management reasons, ordering some type of neuroimaging.
While the patient’s lack of deterioration argues against a lesion that would require intervention, his persistent symptoms probably do increase the chance of some sort of abnormality, which, if discovered subsequently, could be construed as representing poor judgment on the initial clinician’s part. In this situation, discussing the possibilities with the patient, with good documentation and follow-up instructions, is important.
Patient C
The available clinical decision rules indicate that clinicians should maintain a very low threshold for imaging patients over age 60 or 65 who sustain any degree of head impact, even with a normal exam and no worrisome features. If this patient (or a patient of any age) were taking warfarin or an antiplatelet agent (including aspirin), the need for CT scanning is increased to the point that it would be considered necessary. Indeed, the chance of injury in patients who are anticoagulated is high enough that a period of ED or inpatient observation is additionally performed, even after a normal scan, due to the higher probability of delayed bleeding.
References
- National Center for Injury Prevention and Control TBI Centers for Disease Control and Preven- tion website. Available at: www.cdc.gov/ncipc/tbi/TBI.htm. Accessed 11/15/07.
- Dachs RJ, Back E, Glick Emergencies in the office: Why are 911 calls placed from family medicine and ur- gent care offices? J Urgent Care Med. 2007;1(3):19-25. Personal communication with Dr. Dachs, 12/2/07.
- Hoffman JR, Mower WR, Wolfson AG, et Validity of a set of clinical criteria to rule out injury to the cervi- cal spine in patients with blunt trauma. N Engl J Med. 2001;343:94-99.
- Stiell IG, Wells GA, McKnight RD, et Canadian C-spine rule study for alert and stable trauma patients. I. Background and Rationale. Can J Emerg Med. 2002;4:84-90.
- Stiell IG, Wells GA, McKnight RD, et Canadian C-spine rule study for alert and stable trauma patients. II. Study Objectives and Methodology. Can J Emerg Med. 2002;4:185-193.
- American Academy of Practice Parameter: The management of concussion in sports. Available at: www.aan.com/professionals/practice/pdfs/pdf_1995_thru_1998/1997.48.581.pdf. Accessed 1/23/08.
- American College of Sports Medicine, American Academy of Family Practice, American Academy of Orthopedic Surgeons, American Medical Society for Sports Medicine, American Orthopedic Society for Sports Medicine, American Osteopathic Academy of Sports Concussion (mild traumatic brain injury) and the team physician: A consensus statement. Available at: www.acsm.org/AM/Template.cfm?section=Search§ion=Team_Physician_Consensus_Statements&template=/CM/ContentDisplay.cfm&ContentFileID=723. Accessed 1/23/08.
- Macpherson A, Spinks Bicycle helmet legislation for the uptake of helmet use and prevention of head in- juries. Cochrane Database of Systematic Reviews 2007; Issue 2. Art no.: CD005401.
- Liu BC, Ivers R, Norton R, et Helmets for preventing injury in motorcycle riders. Cochrane Database of Systematic Reviews 2004;Issue 2. Art no.: CD004333.
Suggested Reading
- Anderson TA, Heitger M, Macleod AD. Concussion and mild head Practical Neurol. 2006;6:342-357.
- Ropper AH, Gorson Concussion. New Engl J Med. 2007;356(2):166-172.
