Published on
Urgent message: The differential diagnosis of acute orofacial pain is wide ranging; prompt recognition of these syndromes is vital for ensuring the best possible outcome.
John A. Vaughn, MD, Immediate Health Associates, Westerville, OH A cute orofacial pain—pain arising from the teeth or soft tissues of the mouth—is extremely common, affecting 22% of people in the United States. Since it is more likely to affect younger adults and those without adequate access to primary care, it is a frequent presenting complaint in emergency departments and urgent care centers. While there are few true emergencies, the differential diagnosis of acute orofacial pain is wide ranging, and prompt recognition of these syndromes is vital for ensuring the best possible outcome.
This article will provide an introduction to some of the more likely origins of acute orofacial pain, and suggest appropriate management and “next steps” in the urgent care setting.
Dental Pain
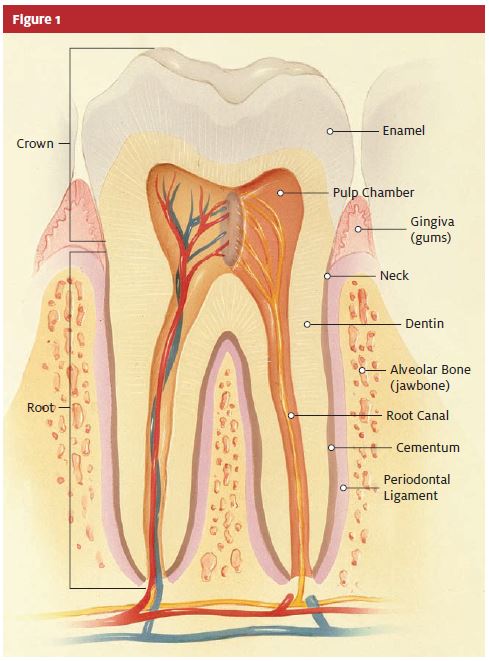
Dental pain is responsible for over 700,000 ED visits a year.2 While non-odontogenic sources such as maxillary sinusitis, migraine headaches, temporomandibular joint (TMJ) syndrome, and neuralgias can cause referred teeth pain, dental sources are the most common. A basic illustration of dental anatomy is presented in Figure 1.
Pathology of Carious Origin
Dietary carbohydrates on the crown surface are metabolized by oral bacteria, most predominantly Streptococcus mutans. Prolonged exposure to these acidic metabolic byproducts leads to an erosion of the enamel layer referred to as dental caries (cavities). Dental caries is treated by removal of the carious tissue and replacement with a filling by a dentist. Dental caries is asymptomatic until the erosion breaches the pulp chamber, when it causes an inflammatory process called reversible pulpitis. Reversible pulpitis is characterized by pain triggered by thermal, sweet, or sour stimuli that typically lasts for only a few seconds. If left untreated, it will progress to irreversible pulpitis, in which the pain is more severe, lasts longer, and is more diffuse.
Continued inflammation will lead to pulp necrosis and apical periodontitis, in which the pain becomes even more severe, will re-localize to the affected tooth, and can be associated with regional lymphadenopathy. Apical periodontitis can become purulent and lead to the formation of an apical abscess, which is often associated with buccal or palatal fluctuance.
Definitive treatment of apical periodontitis and apical abscess is root canal therapy or tooth extraction. Management in the urgent care setting should include providing adequate pain control and arranging follow-up with a dentist within one to two days. If there is evidence of cellulitis, an antistreptococcal antibiotic should be prescribed: penicillin VK 500 mg TID-QID (50 mg/kg divided into three or four doses in children), clindamycin 300 mg QID, or erythromycin 500 mg QID.3
Ludwig’s Angina
A patient whose clinical presentation is consistent with an abscess involving the mandibular teeth should be carefully evaluated for Ludwig’s angina, a potentially life-threatening, rapidly expanding cellulitis of the submandibular and sublingual spaces.
As the floor of the mouth becomes inflamed and indurated, the tongue is elevated and pushed posteriorly leading to airway obstruction. Ludwig’s angina is typically bilateral and patients present with fever, neck swelling, drooling, trismus, pain, dysphagia, and dyspnea.4
The cornerstone of Ludwig’s angina management in the urgent care set- ting is airway protection until the patient can be transported by EMS to an ED for surgical consultation. Treatment involves IV antibiotics, IV steroids, and, if necessary, incision and drainage and surgical decompression with tracheotomy. High-dose penicillin G is the antibiotic of choice, typically administered with an anti- staphylococcal drug and metronidazole for anaerobe coverage.5
Acute Alveolar Osteitis
Acute alveolar osteitis, or dry socket, results from the loss of the protective blood clot that forms in the alveolar socket after a tooth extraction. Patients typically present two to three days postextraction with complaints of acute pain and foul odor. Exam will reveal a dry appearance of the exposed bone in the alveolar socket.
Management is supportive until the patient can follow up with the dentist. The socket can be gently rinsed with warmed saline or chlorhexidine (Peridex) to remove any debris and packed with moistened iodoform gauze or gauze soaked with eugenol. Packing should be changed daily, and appropriate analgesia should be prescribed.
Gingivitis
Chronic accumulation of plaque along the gingival margins in patients with inadequate oral hygiene will lead to inflammation and bleeding. As gingivitis progresses, the inflammation can destroy the periodontal ligament and surrounding alveolar bone. This chronic periodontitis leads to tooth loss and an increased risk of developing acute periodontal abscesses from debris becoming lodged in the periodontal pocket.
Patients with an acute periodontal abscess will typically present with pain, erythema, and edema over the affected segment. The tooth is typically tender to percussion and hyper-mobile. Treatment includes warm saline rinses and referral to a dentist within 24 hours for incision and drainage. If there is any evidence of cellulicellulitis, patients should be started on oral penicillin or erythromycin.
Acute necrotizing ulcerative gingivitis (ANUG, or “trench mouth”) is a rapidly spreading gingival infection caused by an overgrowth of normal oral bacteria including alpha-hemolytic streptococci, Prevotella intermedia, and Actinomyces species. When ANUG spreads beyond the gingiva, it is referred to as noma, or cancrum oris. As an opportunistic infection, ANUG typically affects immunosuppressed patients with poor diet and poor oral hygiene.
Patients usually complain of pain, spontaneous gingival bleeding, foul breath, or alterations in taste. The classic physical findings are gingival edema and ulceration in the interdental papillae (often associated with a gray pseudomembrane), halitosis, and fever.
Treatment includes saline or diluted hydrogen peroxide rinses, topical lidocaine, oral analgesics for pain relief, and oral antibiotics. Penicillin VK is the drug of choice (or erythromycin if the patient is allergic to penicillin). Patients should follow up with a dentist in one to two days.6
Dental Trauma
Dental trauma is extremely common; it is estimated that 50% of all children experience some form of dental trauma.7 Assessment of dental injuries should always include establishing the mechanism and timing of the injury, evaluation for the presence of associated soft tissue injuries or bite malocclusion, and dental radiography to rule out a fracture if available.
Dental Fractures
Dental fractures may involve the crown, root, or alveolar bone. Adequate analgesia should be prescribed and dental follow-up arranged within one to two days. Fractures that expose the pulp may be more painful, but do not necessarily require emergent consultation.
Displacement Injuries
While displacement injuries of primary teeth have min- imal long-term sequelae, displacement injuries of perma- nent teeth are dental emergencies whose prognosis directly correlates with timeliness of treatment.
Intrusive luxation is the displacement of the tooth into the alveolar socket. Since the tooth should be allowed to spontaneously re-erupt prior to any attempts at realignment, tetanus prophylaxis and pain control is all that is required in the urgent care setting. The patient should be non-emergently referred to a dentist for monitoring and potential root canal treatment.
Lateral or extrusive luxation is the loosening and displacement of the tooth within the alveolar socket. In the primary dentition, if the tooth is loose enough that it could be aspirated or cause malocclusion the patient should be referred to a dentist for immediate extraction.8 In the permanent dentition, the patient should be emergently referred to a dentist or oral surgeon for repositioning and splinting. Patients should be placed on appropriate analgesics and antibiotic prophylaxis, and tetanus status addressed.
Avulsion is the complete displacement of the tooth out of the alveolar socket and is a time-sensitive dental emergency; successful reimplantation is less likely if the tooth has been out of the socket for more than 20 minutes.
Primary teeth should never be re-implanted. Permanent teeth should be re-implanted as soon as possible. The tooth should be gently rinsed in sterile saline prior to re-implantation and should only be handled by the crown; any manipulation of the root could disrupt the periodontal ligament fibers that are vital for re-attachment. Antibiotic prophylaxis should be prescribed, tetanus status addressed, and emergent dental consultation for splinting and follow-up management should be made.
If the tooth cannot be rimplanted in the urgent care center, it should be transported with the patient to the consultant in a specialized tooth transport apparatus. If this is unavailable, milk can be used as a transport medium; it is relatively sterile and has pH and osmolality levels compatible enough with periodontal ligament cells to keep them viable for up to three hours.9 Using sterile saline or having the patient carry the tooth in the buccal sulcus is also a reasonable alternative for transport.
Stomatitis
Over a third of acute orofacial pain syndromes are caused by mouth sores.10 While the differential diagnosis is extensive, the following are among the most common causes seen in the urgent care setting.
Oral Candidiasis
Oral candidiasis (“thrush”) is caused by an overgrowth of the ubiquitous fungus Candida albicans.Predisposing factors include: the extremes of age, the use of intra-oral prosthetic devices, recent antibiotic use, and immunosuppression. Patients typically present with white plaques overlying an erythematous base on the buccal mucosa and tongue that can be easily scraped away with tongue depressor. Treatment includes topical or oral antifungal agents, as follows:
- Nystatin (Mycostatin) 100,000 Units/mL. Adults: 4- 6 mL swish and swallow (Infants: 2 mL QID).
- Mycostatin Pastilles 200,000 Units. 1-2 Pastilles dissolved slowly in mouth
- Fluconazole (Diflucan) 200 mg po QD on day 1, then 100 mg po QD for at least 14 days. (Peds: 6 mg/kg po QD on day one, then 3 mg/kg po QD.)
Aphthous Stomatitis
Aphthae are associated with nutritional deficiencies (iron, folate, B-12), Celiac disease, Crohn’s disease and Bechet syndrome, but the etiology of recurrent aphthous stomatitis (RAS, or canker sores) is still unknown. They are extremely painful, well-circumscribed round/oval ulcerations with erythematous borders and yellow or gray bases typically measuring 2-4 mm in diameter.
RAS will resolve spontaneously in seven to 10 days. Topical steroids or viscous lidocaine may be used for supportive care, as follows:
- Dexamethasone (Decadron) elixir 0.5 mg/5 mL. 5 mL swish and spit QAC and
- Triamcinolone (Aristocort) gel 1%; apply two to four times daily.
- Fluocinonide (Lidex) gel 0.5%; apply two to four times
- Lidocaine Viscous 2% gel; apply Q 4 hours
Another treatment option is chemical cautery of the lesion with silver nitrate. This has been shown to reduce pain, although it has no statistically significant effect on healing time.11
Herpes Simplex
Herpes labialis (“fever blisters” or “cold sores”) is caused by the Herpes simplex virus (HSV). The type 1 virus is responsible for the major- ity of cases, but type 2 may also cause oral lesions. Most people have been infected with the virus by adulthood.
HSV stomatitis presents as painful, grouped vesicles on the gingiva, buccal mucosa, lips, or tongue that may extend onto the peri-oral skin. The vesicles quickly rupture to form small ulcerations that will develop a yellow- to honey-colored crust and heal spontaneously over two to three weeks. The pathognomonic feature is a tingling, burning or itching pain that develops in the affected area one to two days before the lesions erupt.
Treatment is supportive. If started during the prodromal phase, antiviral medications have been shown to shorten the course and lessen the severity of the outbreak.
Topical antivirals are much less effective. Typical administration is as follows:
- Acyclovir (Zovirax) 400 mg PO TID (or 800 mg PO BID) for five
- Valacyclovir (Valtrex) 2 g PO Q12 hours for one day (total of 4 g).
Herpangina
Herpangina is an acute febrile illness caused by cox-sackievirus group A that most commonly affects children in the summer months. Patients develop fever, sore throat, headache, cervical lymphadenopathy, and malaise which is followed by the eruption of multiple vesicles on the soft tissues of the posterior pharynx. These vesicles rupture, leaving multiple ulcerations which may last for a week. Unlike herpes labialis and RAS, herpangina lesions do not appear on the gingiva, tongue, or anterior buccal mucosa.
Hand, Foot, and Mouth Disease
Hand, foot, and mouth disease (HFM) is the most common cause of mouth sores in children.12 It is a highly contagious acute febrile illness caused by enteroviruses typically coxsackievirus A16—that usu- ally affects children under the age of 5 with a peak incidence in summer and fall.
After a prodrome of fever, malaise, and sore mouth, painful vesicular lesions that rupture to form shallow ulcers with an erythematous halo will develop on the buccal mucosa, tongue, gingiva, and soft palate. The distinguishing feature of HFM is the presence of a rash on the hands and feet (and often the buttocks). This rash begins as erythematous macules classically on the palmar and plantar surfaces—that progress to gray vesicles on an erythematous base which may be asymptomatic or pruritic.
HFM is self-limited, usually lasting a week, and treatment is supportive.
Angular Cheilitis
Angular cheilitis is a painful inflammation of the corners of the mouth that involves the formation of deep fissures. Angular cheilitis can be the result of an infectious process (usually fungal) or vitamin B deficiency, but is often due to mechanical irritation: thumb sucking in children, lip licking/biting in adults, or excessive pressure in edentulous patients.
Treatment is aimed at correcting the underlying cause, but patients should be encouraged to keep the areas dry and well-lubricated with an emollient.
Leukoplakia
Although leukoplakia rarely causes pain, as a precancerous lesion it should always be included in the differential diagnosis of a patient with oral lesions. It is a thick, rough, hardened, and slightly raised white patch or plaque that develops on the sides of the tongue or buccal mucosa in response to chronic irritation. If the lesion is red, it is referred to as erythroplakia.
Leukoplakia develops over weeks to months and is often asymptomatic. It may become sensitive to touch, heat, or spicy foods. The cause is unknown, but tobacco use especially pipe smoking and the use of chewing tobacco/snuff is associated with a high risk of developing leukoplakia. Unlike oral candidiasis, it is adherent and cannot be easily scraped off with a tongue depressor. The patient with leukoplakia must be non-emergently referred to a dentist or oral surgeon for biopsy evaluation of the lesion. Removal of the underlying irritation may result in complete resolution, but surgical removal of the lesion may be necessary.
Summary
It would behoove the urgent care provider to bear the following key points in mind when treating a patient who has presented with a complaint discussed in this article:
- A patient with an abscess involving the mandibular teeth should be carefully evaluated for Ludwig’s angina, a potentially life-threatening
- Displacement injuries of permanent teeth are dental emergencies whose prognosis directly cor- relates with timeliness of
- Avulsed primary teeth should never be re-impanted
- An avulsed tooth should never be handled by the root, as this could disrupt the periodontal ligament fibers that are vital for re-attachment.
- Any patient with an oral lesion suspicious for leukoplakia/erythroplakia must be referred for biopsy evaluation since this is a pre-cancerous ■
REFERENCES
- Dental, Oral, and Craniofacial Data Resource Oral Health U.S., 2002. Bethesda, Maryland: 2002.
- Lewis C, Lynch H, Johnston B. Dental complaints in emergency departments: a national Ann Emerg Med. 2003;42:93-99.
- Beaudreau Oral and Dental Emergencies. In: Tintinalli JE, Kelen GD, Stapczynski JS, eds. Emergency Medicine: A Comprehensive Study Guide. 5th ed. McGraw-Hill; 2000:1539- 1556.
- Marcincuk M, Murray Deep Neck Infections. Emedicine. Available at:www.emedicine.com/ent/topic669.htm. Accessed December 6, 2006.
- Hartmann Ludwig’s Angina in Children. Am Fam Physician. 1999;60:109-112.
- Stephen Gingivitis. Emedicine. Available at www.emedicine.com/emerg/topic217.htm. Accessed December 8, 2006.
- McTigue Diagnosis and management of dental injuries in children. Pediatr Clin North Am. 2000;47:1067-1084.
- Douglass AB, Douglass JM. Common Dental Emergencies. Am Fam Physician. 2003;67:5111-5116.
- Peng Dental, Avulsed Tooth. Emedicine. Available at www.emedicine.com/- emerg/topic125.htm. Accessed December 8, 2006.
- Dental, Oral, and Craniofacial Data Resource Oral Health U.S., 2002. Bethes- da, Maryland: 2002.
- Alidaee MR, Taheri A, Mansoori P, et Silver nitrate cautery in aphthous stomatitis: a randomized controlled trial. Br J Dermatol. 2005;153:521-525.
- Dyne P, Kesler Devore Pediatrics, Hand-Foot-and-Mouth Disease. Emedicine. Available at www.emedicine.com/emerg/topic383.htm. Accessed December 9, 2006.
