Published on
Urgent message: Lymphadenopathy is a common presenting issue in urgent care. Most cases are benign, but be on the alert for “red flags” that could signal malignancy.
MARIA V. GIBSON, MD, PHD, and DANIEL A. CHERRY, MD
Consider how you would manage the following patient presenting with lymphadenopathy.
A 39-year-old male truck driver presented to the urgent care clinic with a 2- to 3-week history of “swollen glands” in both sides of his groin. They were not painful but “tender to touch.” One week prior, he had a flu-like infection with body aches that had resolved. He had no penile discharge, hematuria or dysuria and no fever, night sweats or weight loss.
Physical examination, including genitalia, was normal except for palpable inguinal lymph nodes (group of 4, 0.5 to 1.0 cm on the right side and two nodes, 3.0 to 4.0 cm in diameter, on left) that were mobile and tender. Urinalysis was normal, as were tests for gonorrhea, chlamydia, HIV, and reactive plasms regain, and herpes simplex virus titer. Inguinal skin KOH prep was positive for fungus. The patient was treated with nystatin powder for tinea cruris. He returned 3 weeks later with persistent pruritic erythema in both sides of his groin and no change in the size or tenderness of the inguinal lymph nodes.
Lymphadenopathy by Definition
Lymphadenopathy is enlargement of one or more lymph nodes. Lymph nodes are considered to be abnormal if one or more is 1.0 cm in diameter, or in the case of an epitrochlear node, > 0.5 cm diameter. Palpability of any lymph nodes in the supraclavicular, iliac, or popliteal regions constitutes lymphadenopathy. The condition can be either localized (single node, group of nodes, or region) or generalized. Generalized lymphadenopathy is established by enlarged nodes in 2 distinct anatomic regions.
Causes and Associated Conditions
Lymphadenopathy is caused by proliferation of lymphocytes and/or associated monocytic/phagocytic cells (reactive or neoplastic) or by infiltration of metastatic malignant cells. In the United States, viral and bacterial infections are the most common etiologies of lymphadenopathy, with infectious mononucleosis (Epstein Barr virus or EBV) and cytomegalovirus (CMV) more frequently associated with generalized lymphadenopathy and beta-hemolytic streptococci more frequently associated with localized lymphadenopathy. In developing countries infections such as HIV, tuberculosis (TB), typhoid fever, leishmaniasis, trypanosomiasis, schistosomiasis and filariasis, and fungal diseases are common causes of lymphadenopathy.
The mnemonic acronym “MIAMI” is often used to remember the broad categories of diseases that present with generalized lymphadenopathy.
- Malignancies (metastasis, lymphomas, skin neoplasms)
- Infections (infectious mononucleosis, pharyngitis, cat-scratch disease, mycobacterial, brucellosis, leishmaniasis, tularemia, toxoplasmosis, CMV, HIV, viral hepatitis, TB, syphilis, lymphogranuloma venereum rubella)
- Autoimmune disorders (systemic lupus erythematosus, rheumatoid arthritis, dermatomyositis, Sjogren syndrome)
- Miscellaneous (sarcoidosis, Kawasaki disease)
- Iatrogenic (medications, hyperthyroidism, serum sickness, severe hypertriglyceridemia); numerous unusual systemic diseases (pneumoconiosis, lysosomal storage diseases, Castleman’s disease, Kimura’s disease, Rosal-Dorfman disease, Kikuchi’s lymphadenitis [histiocytic necrotizing lymphadenitis]).
Adverse drug reactions (allopurinol, atenolol, captopril, cephalosporins, carbamazepine, hydralazine, penicillins, primidone, pyrimethamine, phenytoin, quinidine, trimethoprim/sulfamethoxazole, sulindac) can cause generalized lymphadenopathy that may be associated with a rash, fever, hepatosplenomegaly, jaundice, and anemia. A common example of such reactions can occur in patients a few weeks after taking phenytoin.
Lymphadenopathy Presentation
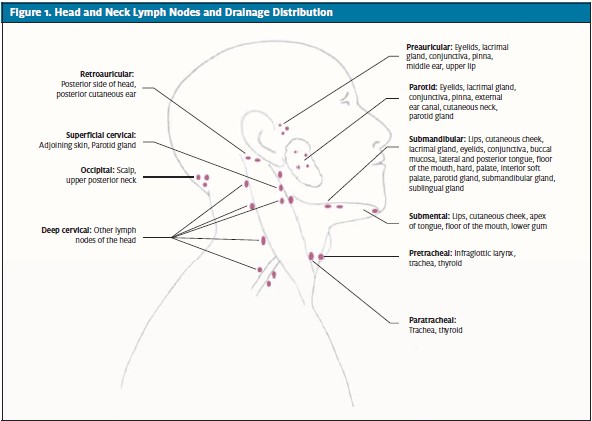
The occurrence of lymphadenopathy is disease-dependent and the cause often is obvious after a complete history and physical examination. Patients may present with general symptoms: fever, chills, night sweats, weight loss (infection/lymphoma “B” symptoms), easy bruising (lymphoma occupying the bone marrow), new skin lesions (infections or neoplastic), jaundice (hepatitis), or arthritis (lupus or rheumatoid arthritis). Exposure to household pets, diseases, travel history, history of trauma or injury, or new medications provide key information relevant to the diagnosis of lymphadenopathy. At the time of physical examination, all major palpable lymph node groups should be examined to evaluate for generalized lymphadenopathy because of its common association with serious systemic diseases (Figures 1 and 2). Assessment of the size, location, distribution, and character of the lymph nodes is essential. Painful and tender lymph nodes are often signs of localized infection. Inflamed lymph nodes due to local staphylococcal and streptococcal infections may progress to fluctuation, especially in children, and require incision and drainage and antibiotic administration. Multiple enlarged cervical nodes that develop over time and become fluctuant without significant inflammation or tenderness, with or without fever, suggest infection with Mycobacterium TB, atypical mycobacteria or Bartonella henselae (cat scratch disease).
Lymph nodes that are hard on palpation and nontender, particularly in older patients and in smoker, are suggestive of metastatic cancer (such as of the oropharynx, nasopharynx, larynx, thyroid, and esophagus). These patients should be referred to an otolaryngologist for upper airway endoscopy. Hard and painless lymph nodes are also seen with sarcoidosis. Bilateral, mobile, nontender lymphadenopathy may be associated with viral infection. Keep in mind that palpable “lymph nodes” may mimic other masses, such as brachial cleft cysts and other benign tumors.
Localized Lymphadenopathy
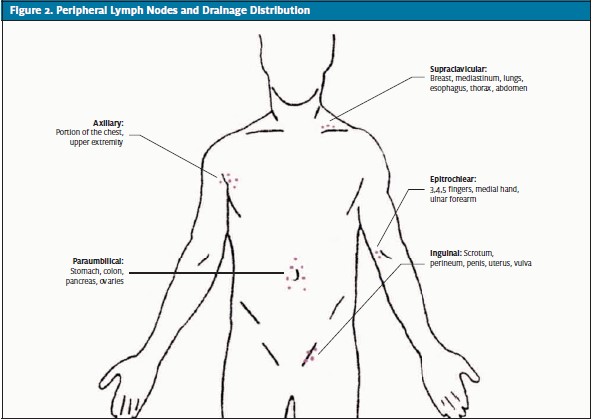
The anatomic arrangement and drainage distributions of the major palpable lymph nodes are shown in Figures 1 and 2.
In patients with cervical lymphadenopathy, thorough examination of the mouth, oropharynx, nose, and ears is essential. Submandibular lymphadenopathy is usually caused by infections of the head, sinuses, ears, eyes, scalp, mouth, pharynx and neck. Enlargement of submental lymph nodes is due to systemic infections such as infectious mononucleosis is most common in patients with pharyngitis and rubella. Other viral causes of cervical lymphadenopathy include adenovirus, herpesvirus, coxsackievirus, HIV, and CMV. Bacterial infections may be localized within the lymph nodes themselves (lymphadenitis). Posterior cervical lymph node enlargement is often due to infection (EBV, TB), and less frequently to head and neck malignancies (lymphomas or metastatic squamous cell carcinoma). Subocipital and post- and pre-auricular lymph nodes become enlarged with infections of the scalp or ear. The supraclavicular nodes are particularly important because their enlargement is strongly suggestive of metastatic malignancy.
Right supraclavicular lymphadenopathy may represent metastasis from the lung, retroperitoneum or gastrointestinal tract. In patients with left supraclavicular lymphadenopathy lymphoma, metastatic thoracic or retroperitoneal cancer and fungal infection should be excluded. Axillary lymph nodes enlargement can potentially be due to local infections, cat scratch disease, lymphoma, breast cancer, silicone implant leakage, brucellosis, or melanoma. Hidradenitis suppurative is a condition of enlarged tender lymph nodes that typically affects patients with obesity and includes recurrent abscesses of lymph nodes in the axillary chain, which may require treatment with incision and drainage and a course of antibiotics. Patients with epitrochlear lymphadenopathy, depending on history, should be evaluated for local infections, lymphoma, sarcoidosis, tularemia, and secondary syphilis. Enlarged periumbilical (Sister Mary Joseph) nodes are strongly associated with carcinoma, especially that of the pancreas.
Inguinal lymph nodes up to 1 to 2 cm in size are common in otherwise healthy adults and generally have a low suspicion for malignancy. Sexually transmitted infections (herpes simplex virus, gonococcus, syphilis, chancroid, granuloma inguinale, lymphogranuloma venereum), infections of the lower extremity, lymphoma, and pelvic malignancies are potential causes of inguinal lymphadenopathy. Primary malignancies of the skin of the lower extremities, cervix, vulva, skin of the trunk, rectum, anus, ovaries and penis may metastasize to the inguinal lymph nodes. In addition to palpation of the major lymph node groups, examination of the skin for malignancies (melanoma, Kaposi sarcoma) and infection is essential. Abdominal examination can reveal splenomegaly, which can be a sign of lymphoma or infectious mononucleosis.
Lymphadenopathy and Malignancy
In one model, clinical characteristics reported to predict the likelihood of malignancy in adults with lymphadenopathy included age > 40 years, presence of other physical signs, abnormal CBC, abnormal liver function tests, negative Mantoux test, and generalized lymphadenopathy (multivariate predictor only). Additional evidence suggesting malignancy includes fixed, firm nodal character, duration of more than 2 weeks, and supraclavicular or periumbilical location. “Red flags” that should raise suspicion of malignancy are listed in Table 1.
Lymphomas are clonal neoplasms of B lymphocytes, T lymphocytes, and natural killer (NK) cells. In addition to lymphomas, a number of non-lymphocytic hematologic neoplasms can occur in lymph nodes such as those of histiocytes and Langerhan cells. Although lymphomas comprise approximately 40 major entities plus subtypes, a few generalizations can be made:
Indolent lymphomas usually presents with more widespread (generalized) involvement than more aggressive lymphomas.
Non-Hodgkin lymphomas are most common in the upper middle age group and the elderly, lymphomas in young adults are most often Hodgkin lymphoma, and in infants and young children, lymphoblastic lymphoma is most prevalent.
Aggressive lymphomas are more often curable while indolent forms are usually chronic and incurable and may or may not significantly shorten the patient’s lifespan, with or without treatment.
| Table 1. Red Flags for Malignancy | |
| Red Flags | Clinician Alert |
| History Older age, duration of lymphadenopathy > 4 weeks, absence of infections, exposure to animals and insects, chronic use of medications, personal or family history of malignancy |
Increased risk of malignancy |
| Recurrent fever, night sweats, and unexplained weight loss > 10% | Suspicious for Hodgkin and non-Hodgkin lymphoma Environmental tobacco, alcohol, and ultraviolet radiation exposure |
| Suspicious for metastatic carcinoma of the lung, esophagus, stomach, liver, or cancers of the head and neck, and skin. | Patients who are immunocompromised and HIV-positive increased risk of Kaposi sarcoma and non-Hodgkin lymphoma |
| Pain in the area of lymphadenopathy after even limited alcohol ingestion | Specific finding for Hodgkin lymphoma |
| Exam Lymph nodes that are firm, fixed, circumscribed, and painless |
Increased significance for malignant or granulomatous disease; further investigation necessary |
| Supraclavicular lymphadenopathy | Most likely consistent with malignancy, and should always be investigated and biopsied, even in children |
| Palpable anterior and central axillary lymph nodes with lack of infection exposure | Suspicious for metastatic breast adenocarcinoma |
| Antecubital or epitrochlear lymphadenopathy | May suggest lymphoma or melanoma |
| Persistent inguinal lymphadenopathy with negative STD testing and absence of skin infection signs | Consider investigation for Hodgkin and non-Hodgkin lymphomas, penile, testicular and vulvar carcinomas, and melanoma |
| Any unexplained, non-inguinal lymphadenopathy lasting > 4 weeks | Consider specific investigation and/or biopsy |
Keys to Evaluation of Lymphadenopathy
Additional testing must be driven by the clinical evaluation, as described in Table 2.
Examination of peripheral blood is an important element of lymphadenopathy evaluation. The automated WBC and differential cell counts may reveal neutrophilia in support of an infectious or reactive process, lymphocytosis hinting at a viral illness or lymphoma, or cytopenias raising suspicion for involvement of the bone marrow by lymphoma. Abnormal automated blood counts in the context of lymphadenopathy should prompt a request to have the peripheral blood smear examined by a pathologist. Biytopenia or pancytopenia is particularly suspicious for bone marrow occupying disease. The erythroid sedimentation rate is a good general screening study for rheumatologic disease, which can be followed by specific serology as clinically indicated. Suppurative or necrotizing lymphadenitis should be evaluated with culture. Serologic tests are best for assessing for the possibility of CMV, EBV, and toxoplasmosis. An acid-fast bacillus smear, serum calcium, and serum angiotensin converting enzyme (ACE) levels may be helpful in the setting of granulomatous lymphadenitis (calcium and ACE may be elevated with sarcoidosis). Regarding reactive causes of lymphadenopathy, the pathologic findings are commonly nonspecific and rarely lead to a specific etiology.
| Table 2. Considerations for Laboratory Testing for Lymphadenopathy |
|
| Abbreviations: ACE = angiotensin converting enzyme, AFB = acid fast bacilli, ANA = antinuclear antibodies, CBC = complete blood count, CMV = cytomegalovirus, EBV = Epstein-Barr virus, ESR = erythrocyte sedimentation rate, LDH = lactate dehydrogenase, PCR = polymerase chain reaction, RF = rheumatoid factor, RPR = reactive plasmin regain, TB = tuberculosis, VDRL = venereal disease research laboratory |
Management
The first step in evaluation of lymphadenopathy is to assess the patient for the most common viral/bacterial infections and medication side effects. Risk factors for, exposure to, and generalized symptoms of systemic infections should be evaluated. If the findings suggest a benign etiology that is usually self-limited, then reassurance can be provided to the patient. Benign reactive adenopathy can be safely observed for months if there is no suspicion of malignancy. Follow up should be scheduled if the lymphadenopathy is persistent and/or a systemic cause is suspected. There are no evidence-based guidelines for the appropriate observation period but many authors justify a 3- to 4-week period after which biopsy is warranted. If malignancy is a serious consideration, biopsy should be done more urgently.
Treatment with antibiotics followed by reevaluation in 2 to 4 weeks is indicated if clinical findings suggest lymphadenitis. Consultation with a clinical hematologist, otolaryngologist, or surgeon should be requested when malignancy is suspected. Consultation with an infectious disease specialist may be warranted in cases of generalized lymphadenopathy that are resistant to antibiotic treatment or when systemic infections such as brucellosis, leishmaniasis, tularemia, toxoplasmosis, or HIV are suspected.
Patient Education
Most of the time lymphadenopathy is a benign condition caused by bacterial or viral infection, but it can sometimes be a sign of malignancy, serious infection or drug reaction. Therefore, follow up with a health care provider in 1 to 2 months is imperative. Advise patients to follow up earlier if fever lasts longer than 24 hours, lymph nodes increase in number or size, tenderness increases, or other symptoms occur.
Bibliography
- Abba AA, Bamgboye EA. Predicting nodal malignancy from clinical data. Saudi Med J. 2003; 24(7): 769-773.
- Bazemore AW, Smucker DR. Lymphadenopathy and malignancy. Am Fam Physician. 2002; 1; 66(11): 2103-2110.
- Evaluation of Lymphadenopathy. In: Goroll AH, Mulley AG, eds. Principles of Primary Care, 5th Philadelphia: JB Lippincott, 2005: 73-77.
- Fijten GH, Blijham GH. Unexplained lymphadenopathy in family practice. An evaluation of the probability of malignant causes and the effectiveness of physicians’ workup. J Fam Pract 1988; 27: 373-376.
- Karaman AE, Karaman I, Cavusoglu YH, Erdogan D. The ongoing problem with peripheral lymphadenopathies: which ones are malignant? Pediatr Surg Int. 2010; 26: 247-250.
- Kliegman RM, Nieder ML, Super DM. Lymphadenopathy. In: Fletcher J, Bralow L, eds. Practical Strategies in Pediatric Diagnosis and Therapy. WB Saunders Co; 1996; 791-803
- Larsson LO, Bentzon MW, Berg Kelly K, et al. Papable lymph nodes of the neck in Swedish schoolchildren. Acta Paediatr. 1994; 83(10): 1091-1094.