Published on
Differential Diagnosis
- Osteolytic lesion
- Lateral condyle fracture
- Elbow dislocation
- Radial head fracture
- Fat pad sign
Physical Examination
Examination reveals the following:
Vitals: Afebrile, pulse 88, respirations 20, BP 92/76
General: Alert and oriented, no acute distress, facial grimace
Lungs: Clear to auscultation bilaterally
Cardio: Regular rate and rhythm without murmur, rub, or gallop
Abdomen: Soft and nontender without rigidity, rebound, or guarding. No bruising or distention
Extremities: There is pain with palpation over the right elbow
Physical exam reveals the patient is in significant pain. Tachycardia may be present from the pain or from an associated injury. The patient will have tenderness with palpation over the lateral aspect of the elbow and decreased range of motion. Check sensation and peripheral pulse.
Diagnosis
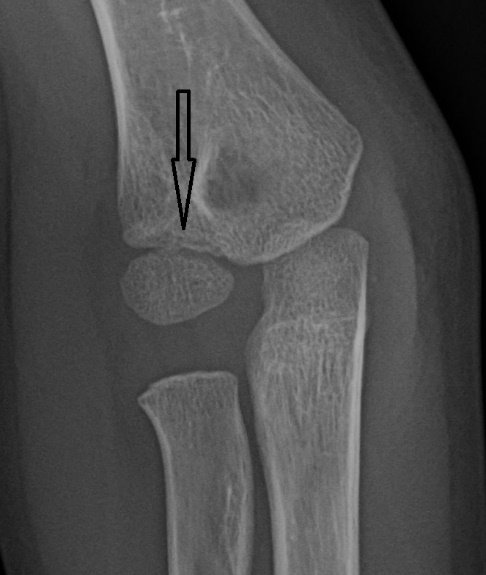
The x-ray reveals a fracture of the lateral humeral condyle. Subtle curvilinear lucency is seen at the distal margin of the lateral humeral condyle. Capitellum appears normal. No joint effusion is apparent.
Learnings
A pediatric condyle fracture is one of the most common fractures, accounting for 20% of elbow fractures. The findings are often subtle, but it is an important fracture to diagnose. The mechanism often occurs after a fall onto an outstretched hand, typically with the forearm in abduction and the elbow in extension. It occurs most often between the ages of 6 and 10. Injuries may also involve the brachial artery and the ulnar nerve.
The elbow is composed of the distal humerus, the radial head, and the olecranon (proximal ulna). The capitellum is the distal aspect of the lateral humerus. It is typically displaced posteriorly with a supracondylar fracture, from force applied down the radius (eg, a fall on an outstretched hand will transmit force down the radius causing the proximal radius to “push” the capitellum posteriorly). In the normal elbow, a line drawn along the anterior aspect of the humerus should intersect the middle 1/3 of the capitellum. If the capitellum is fractured, it will be displaced posteriorly, and the “anterior humeral line” will not transect the capitellum.
What to Look For
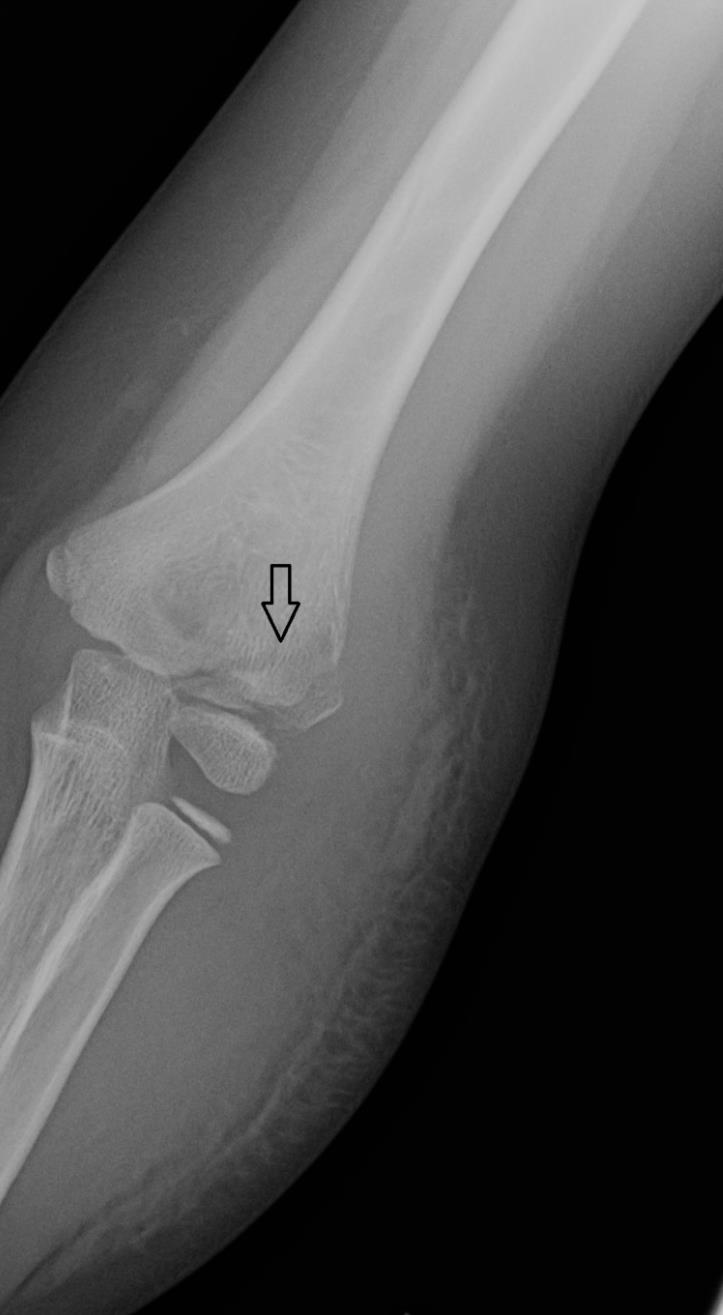
Testing initially involves a plain x-ray series. The x-ray above has a subtle finding, demonstrated by an arrow which reveals a lucency. Other x-ray findings include the presence of a “fat pad” sign. A line should be drawn on the anterior aspect of the humerus to ensure it transects the middle 1/3 of the capitellum. An easy way to remember this finding is keep in mind a common mechanism of lateral condyle fracture: a fall on the outstretched hand transmits energy up the radius placing pressure, which results in displacement of the capitellum posteriorly. When the “anterior humeral line” is drawn, the capitellum will be posterior to the line. The x-ray below demonstrates a much more obvious fracture.
Inquire about the mechanism, which will often be from a fall onto an outstretched hand. The patient will have elbow pain, increased with range of motion. Inquire about paresthesias which may be from injury to the ulnar nerve or brachial artery, pain in the joint above and below, as well as other injuries which may have been sustained.
Treatment
In the urgent care center, initial management involves adequate analgesia and immobilization. Fractures of the lateral condyle of humerus are unstable even when immobilized. These fractures are also prone to nonunion since the fracture is intraarticular and is bathed in synovial fluid. The arm should be placed in a sling and swathed for comfort, with the patient referred to an orthopedic surgeon for follow-up.
Indications for transfer include the following:
- Open fractures
- Concerning mechanism of injury, such as major trauma from a motor vehicle collision
- Consideration of abuse
- Vascular or nerve injury
- Unstable vital signs