Published on
Urgent Message: Isolated sternal fractures in children can occur from relatively minor trauma, such as a trampoline fall, and patients can often be managed conservatively.
NaShayla Davis, MD; Olabisi Pearse, MD; Swati Mahajan, MD; Marie-Helene Gagnon, MD; Rebecca Burger, MD
Citation: Davis N, Pearse O, Mahajan S, Gagnon MH, Burger R. Isolated Sternal Fractures After Trampoline Falls in Children: A Case Series. J Urgent Care Med. 2024; 18(6): 13-16
Key Words: Trampoline, Fall, Fracture, Injury, Case Report
Abstract
Introduction: Trampoline use among children has increased in recent decades. Isolated sternal fractures are an overall uncommon pediatric injury. The limited data in the literature on isolated sternal fractures in children suggest that the injury may not necessitate extensive additional work-up as would be the case if sternal fracture occurred in a multi-injured patient.
Clinical Presentation: We present a case of an isolated sternal fracture secondary to trampoline use, in which a 7-year-old boy presented with chest pain after falling from a zip line onto a trampoline.
Physical Exam: The patient had no external signs of trauma, but he did have tenderness with palpation of the sternum.
Case Resolution: A sternal x-ray demonstrated a buckle fracture, which was managed conservatively, and the patient recovered uneventfully.
Conclusion: It is important to be aware that isolated sternal fractures can occur from relatively minor trauma in children, such as trampoline or bounce-house falls. A sternal fracture from such a mechanism of injury typically does not have associated intrathoracic injuries, and patients can usually be managed conservatively with minimal work-up.
Introduction
Trampoline use has increased in popularity over recent decades with the rise in commercial trampoline parks, which has resulted in greater numbers of associated injuries. From 2000-2005 there were, on average, more than 88,000 pediatric trampoline-related injuries that presented to emergency departments (EDs) annually in the United States.[1] Injuries in children resulting from trampoline use can range from fractures to sprains/strains to simple contusions and abrasions. Sternal fractures have also been described as a type of injury which can result from trampoline play in children.[2]
Sternal fractures most commonly occur from direct trauma to the anterior chest, but can occur without direct trauma as well, with motor vehicle collisions (MVCs) being the most common culprit.1 Trauma resulting in sternal fracture can also be associated with other thoracic pathology, such as acute respiratory distress (ARDS) and pulmonary contusions.[3],[4] An isolated sternal fracture can actually occur from relatively minor trauma, however, and is less commonly associated with intrathoracic complications.5 Patients with an isolated sternal fracture can be managed conservatively and can generally be safely discharged without continuous cardiac monitoring.[5],[6] There are relatively few reports of isolated sternal fractures in children in the literature, but none of which were secondary to trampoline use. In addition to the case presented, there have been several other children over the past 5 years who presented to our hospital system with isolated sternal fractures related to either trampoline or bounce house use.
Clinical Presentation
A 7-year-old male presented to the pediatric emergency department with chest pain after letting go of a zip line onto a trampoline the day prior. He landed on his side and had no loss of consciousness. The patient complained of sternal pain after the fall.
Physical Exam Findings
On examination, the patient was awake and in no acute distress. His vitals were stable. The airway was patent and clear. His lung sounds were symmetric and clear without wheezes, rales, or rhonchi. On cardiac auscultation, he had normal S1 and S2, regular rate and rhythm, no murmurs, and normal pulses and capillary refill. He had normal mental status and no focal neurologic deficits. The patient had no external signs of trauma (eg, abrasions, ecchymoses, swelling). His abdomen was soft, non-tender, non-distended, with normal active bowel sounds, without rebound or guarding. There was tenderness to palpation over the upper sternum without crepitus or deformity. There was no tenderness or deformity of the clavicles. He had normal range of motion without tenderness or swelling in all 4 extremities.
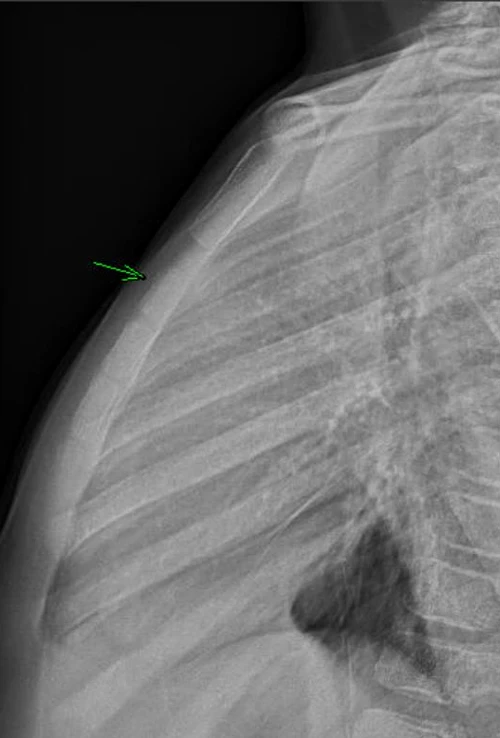
a Buckle Fracture
Diagnostic Assessment
Based on chest exam findings, a sternum radiograph was obtained. The sternum radiograph showed a buckle fracture of the sternum (Figure 1).
Therapeutic Intervention and Case Conclusion
The patient’s family was advised to apply ice to the chest, use ibuprofen as needed, and to avoid strenuous activity for the next several weeks. Return precautions were discussed, and pediatrician follow-up was recommended for recheck. At follow-up, the patient had no complications resulting from the injury.
Case Discussion
This case demonstrates an uncommon musculoskeletal injury that can result from trampoline use. Sternal fractures are thought to be uncommon in children due to the increased elasticity and pliability of their chest wall, which reduces the likelihood of fracture.5 Sternal fractures in children are usually the result of severe blunt trauma to the chest, such as with a motor vehicle collision.3,4 Isolated sternal fracture in children, however, has also been described after relatively minor trauma,5 such as from a trampoline or bounce-house fall as seen with this patient.
Recreational trampoline use has gained popularity in the United States over recent decades. The American Academy of Pediatrics released a policy statement in 2012 recommending that pediatricians counsel patients and families against recreational trampoline use, regardless of safety measures, such as enclosures.[7] According to the US Consumer Product Safety Commission’s National Electronic Injury Surveillance System for 2021 the rates for trampoline injury were 132 per 100,000 for 0- to 4-year olds and 171 per 100,000 for 5- to 14-year olds.[8] Of those pediatric patients who sustain trampoline-related injuries, lighter children are more than 13 times more likely to sustain an injury compared to heavier children, which may be due to less complete motor development.[9],[10] The risk of injury also increases with more participants on the trampoline.10
Isolated sternal fractures caused by a trampoline fall typically occur in toddler and school-aged children.[11] Previous studies focusing on isolated sternal fractures in a large cohort of pediatric patients from a variety of low energy mechanisms, including a trampoline fall, did not find an association with blunt cardiac injury (BCI).5,11 Patients who sustain a major chest injury, such as those related to high velocity MVC, however, do have an increased risk for BCI and other significant intrathoracic and intraabdominal injuries and warrant further work-up.[12]
The Eastern Association of Surgeons for Trauma guidelines suggest an electrocardiogram (ECG) and troponin blood test are reasonable to screen for BCI in adult patients who sustain a sternal fracture, though these recommendations have softened in recent iterations.[13] The utility of obtaining these studies in children is even less clear, but studies have generally not supported an association between isolated sternal fractures in children with low energy mechanisms and BCI.11 Therefore, strong recommendations for or against obtaining ECG and troponin blood tests in pediatric patients who sustain minor chest wall injuries have been avoided.5,11
Case Series Methods and Inclusion Criteria
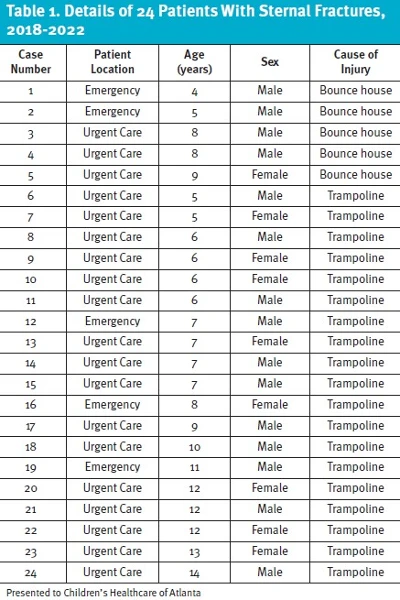
Upon review of patients from our institution from 2018-2022, we found 24 patients via retrospective chart review (median age 7.5 years, 62% male) with sternal fractures resulting from a trampoline or bounce-house injury who presented to either the ambulatory urgent care sites or the ED (Table 1). Cases were identified by searching our institutional database of radiographs for patients under the age of 21with radiologic findings of sternal fractures from 2018-2022. Chart review was then performed on potential cases and only cases with confirmed history of “trampoline” or “bounce house” mechanisms of injury were included. Patients with other mechanisms of injury were excluded. All patients had chest or sternal x-rays, which showed an isolated sternal fracture. Of the 24 sternal fractures, only 1 was noted to be minimally displaced, while 13 were documented as buckle fractures, and the remaining 10 were documented as non-displaced.
Nine of 24 patients (37.5%) had an ECG ordered (mean age of 7.6 years), 7 of 9 (77.8%) of which were normal (mean age of 8 years). The other 2 patients with abnormal ECG findings followed up with a cardiologist and all were subsequently cleared (mean age of 6.5 years). There were 11 of 24 (45.8%) referred to orthopedics for outpatient follow up (mean age of 9.1 years). One patient returned to urgent care with a request for sports clearance. Most patients were discharged directly from the ED or urgent care.
Two of the 24 patients were admitted to the hospital (mean age of 7.5 years), both of which presented to the ED initially. The first patient presented to the ED for chest pain after falling out of a bounce house onto a wooden floor but had no tenderness to palpation on initial exam or complaint of pain. This patient was admitted per surgery recommendations despite having normal ECG, troponin, and no pain. The reason for admission was not clear from chart review, however, he was discharged the following day. The other patient presented for chest pain along with head injury and was noted to have a T6 compression fracture on their chest x-ray along with a sternal fracture. This patient was admitted for IV analgesia as the pain was not adequately controlled with oral agents. This patient was discharged the following day and did not require any surgical intervention. This was the only patient of the 24 patients in this series who had any fracture beyond an isolated sternal fracture.
Discussion and Summary
Our reported number of isolated sternal fractures likely underestimates the incidence of sternal fractures resulting from trampoline or bounce-house injuries seen in our facilities. Only patients who presented to the ED or urgent care centers within our institution who had a chest or sternal x-ray showing a sternal fracture and had documentation of a trampoline or bounce-house injury were included. This likely does not represent all pediatric patients in our area who have had sternal fractures related to trampolines or bounce houses as patients were not included if the mechanism was not noted, if patients sought care outside our institution or at their primary care provider’s office, or if they did not undergo any medical evaluation.
Although sternal fractures are an uncommon injury in the pediatric population, clinicians should be aware that this is an injury that can occur from relatively minor trauma, such as a trampoline or bounce-house fall. As with all injuries, it is important to do a thorough physical exam to rule out other associated injuries. A sternal fracture from this type of injury typically does not have associated intrathoracic injuries, and patients can be managed conservatively with minimal work-up. Patients should be advised to follow up with their pediatricians, use non-steroidal anti-inflammatory drugs as needed for pain, and refrain from rigorous exercise for 4-6 weeks. Strict return precautions should be discussed.
Ethics Statement
The specific patient was unable to be contacted as he was lost to follow-up, and therefore demographics and some details of the case were changed to protect patient anonymity and confidentiality. In the case series review, specific patient identifiers were also intentionally omitted for patient privacy. This case review was part of a quality project, and therefore no institutional review board approval was required as it did not fall under human subjects research.
Take Away Points
- Sternal fractures do occur but are an uncommon injury in the pediatric population.
- A sternal fracture can occur from relatively minor trauma, such as a trampoline or bounce-house fall.
- Isolated sternal fractures from this type of injury almost never have associated intrathoracic injuries and therefore can be managed conservatively with minimal work-up, including a chest or sternal x-ray without a need for obtaining an ECG.
Manuscript submitted July 10, 2023; accepted February 2, 2024.
Author Affiliations: NaShayla Davis, MD, Pediatrics, Emory University School of Medicine; Emergency Medicine, Children’s Healthcare of Atlanta. Olabisi Pearse, MD, Children’s Healthcare of Atlanta; Swati Mahajan, MD, Children’s Healthcare of Atlanta. Marie-Helene Gagnon, MD, Pediatrics, Emory University School of Medicine, Radiology, Children’s Healthcare of Atlanta. Rebecca Burger, MD, Pediatrics, Emory University School of Medicine, Emergency Medicine, Children’s Healthcare of Atlanta. Authors have no relevant financial relationships with any ineligible companies.
References
- [1]. Linakis JG, Mello MJ, Machan J, Amanullah S, Palmisciano LM. Emergency department visits for pediatric trampoline-related injuries: an update. Acad Emerg Med. 2007;14(6):539-544. doi:10.1197/j.aem.2007.01.018
- [2]. Hussein MH, Toreih AA, Attia AS, et al. Trampoline Injuries in Children and Adolescents: A Jumping Threat. Pediatr Emerg Care. 2022;38(2):e894-e899. doi:10.1097/PEC.0000000000002457
- [3]. Perez MR, Rodriguez RM, Baumann BM, et al. Sternal fracture in the age of pan-scan. Injury. 2015;46(7):1324-1327. doi:10.1016/j.injury.2015.03.015
- [4]. Rosenfeld EH, Lau P, Shah SR, et al. Sternal fractures in children: An analysis of the National Trauma Data Bank. J Pediatr Surg. 2019;54(5):980-983. doi:10.1016/j.jpedsurg.2019.01.031
- [5]. Ferguson LP, Wilkinson AG, Beattie TF. Fracture of the sternum in children. Emerg Med J. 2003;20(6):518-520. doi:10.1136/emj.20.6.518
- [6]. Sadaba JR, Oswal D, Munsch CM. Management of isolated sternal fractures: determining the risk of blunt cardiac injury. Ann R Coll Surg Engl. 2000 May;82(3):162-6. PMID: 10858676; PMCID: PMC2503430.
- [7]. Council on Sports Medicine and Fitness, American Academy of Pediatrics, Briskin S, LaBotz M. Trampoline safety in childhood and adolescence. Pediatrics. 2012;130(4):774-779. doi:10.1542/peds.2012-2082
- [8]. National Electronic Injury Surveillance System (NEISS). U.S. Consumer Product Safety Commission. Accessed March 7, 2023. https://www.cpsc.gov/library/neiss.html
- [9]. Choi ES, Hong JH, Sim JA. Distinct features of trampoline-related orthopedic injuries in children aged under 6 years. Injury. 2018;49(2):443-446. doi:10.1016/j.injury.2017.12.017
- [10]. Hurson C, Browne K, Callender O, et al. Pediatric trampoline injuries. J Pediatr Orthop. 2007;27(7):729-732. doi:10.1097/BPO.0b013e318155ab1
- [11]. Chalphin AV, Mooney DP. Pediatric sternal fractures: A single center retrospective review. J Pediatr Surg. 2020;55(7):1224-1227. doi:10.1016/j.jpedsurg.2019.10.002
- [12]. Ramgopal S, Shaffiey SA, Conti KA. Pediatric sternal fractures from a Level 1 trauma center. J Pediatr Surg. 2019;54(8):1628-1631. doi:10.1016/j.jpedsurg.2018.08.040
- [13]. Clancy K, Velopulos C, Bilaniuk JW, et al. Screening for blunt cardiac injury: an Eastern Association for the Surgery of Trauma practice management guideline. J Trauma Acute Care Surg. 2012;73(5 Suppl 4):S301-S306. doi:10.1097/TA.0b013e318270193a
Click Here to download the article PDF