Published on
Denials and rejections are inevitable in medical billing and can have drastic repercussions on the overall profit of an urgent care practice. Studies show almost 30% of medical bills are prone to errors. Avoid these common mistakes to improve the return on your investment.
Eligibility Errors
Avoidable eligibility errors are the biggest issue in urgent care billing. Over one-third of total visits with a rejection or denial are due to a lack of proper registration and/or eligibility verification. Many clinics utilize real time eligibility (RTE) at a high rate but fail to identify potential issues within the responses.
Eligibility errors are largely simple and avoidable but are costly. According to Medical Group Management Association (MGMA), the cost to rework the average denial or rejection is $25. Additionally, visits that incur a front-end rejection or denial are 46% more likely to result in bad debt.
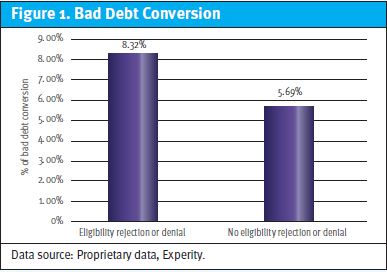
Don’t assume active coverage equals a clean eligibility response. Many eligibility rejections or denials are received even after receiving an “active coverage” RTE response. For example, patients with active Medicaid coverage may be covered by a Managed Medicaid plan, which should be the plan used during registration as opposed to the state Medicaid plan. See Figure 1 for a comparison of bad debt conversion with eligibility rejection or denial vs claims where there is no eligibility rejection or denial.
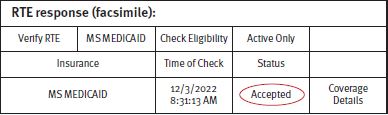
In this example, the RTE response indicates the patient is active with Mississippi Medicaid. However, the patient actually has a United Healthcare Community Plan, which is a Managed Medicaid plan in Mississippi.
Train your front desk to identify Managed Medicare and Medicaid plans in your area. Medicare patients are instructed by the Center for Medicare & Medicaid Services (CMS) to present both their traditional Medicare card and their Managed Medicare card, which can cause confusion. Go beyond asking the standard Has anything changed? question. Best practice is to ask for the insurance card and run RTE at every visit.
As of April 1, 2023, states will be able to start processing Medicaid redeterminations and disenrolling residents who no longer qualify. They will have 14 months to review the eligibility of their beneficiaries. As part of the COVID-19 relief package passed in March 2020, states were barred from terminating members from Medicaid during the public health emergency (PHE) in exchange for additional federal matching funds.
Roughly 15 million people could be dropped from Medicaid when the continuous enrollment requirement ends, according to an analysis the Department of Health and Human Services released in August 2022.
Not Collecting Patient Responsibility
Patient balances accounted for 30% of the total amount owed to urgent care operators in 2021, but represent nearly all the bad debt. This number was higher in years prior to COVID-19, but will increase once the PHE ends on May 11, 2023.
Ensure copayments are collected, review existing balances, and implement or enhance your credit card on file (COF) protocol.
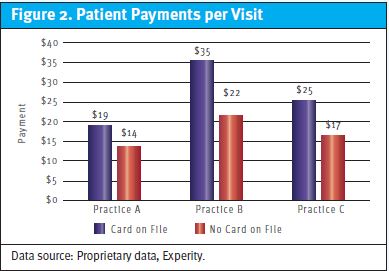
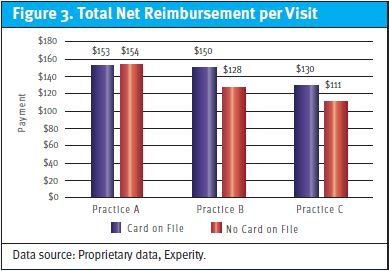
Figure 2 and Figure 3 represent a total of 488,000 fully adjudicated visits from 2021 where BCBS was the primary provider.
In March 2022, the national credit reporting agencies (CRAs) Equifax, Experian, and TransUnion announced joint measures that would result in nearly 70% of paid medical debt tradelines being removed from consumers’ reports. This includes three major components:
- Effective July 1, 2022, the CRAs will no longer include on consumers’ credit reports any medical debt that has been paid in full after being sent to collections.
- Effective July 1, 2022, unpaid medical bills cannot be reported until they are at least 365 days past the date of first delinquency.
- On March 30, 2023, the CRAs will no longer include on consumer reports any medical debts with an original balance less than or equal to $500.
Analysis shows that 95% of urgent care patient balances are less than $500. These new rules remove the incentive for patients to pay their balances once they leave the office, as there are no repercussions
Incorrect Coding
Improper coding impacts clean claims, causes denials or rejections, and results in costly rework. Once a claim is denied by an insurance plan, it takes up to five times the work to get payment.
Proper and thorough coding will increase clean claim rate and potentially improve net reimbursement per visit (NRPV) by allocating the correct E/M levels. Consider utilizing a differential diagnosis when appropriate. This may support the complexity of the problem addressed and is a tool to document the provider’s thought process.
Other common coding errors are the use of unspecified diagnosis codes and not using modifiers for laterality. While an unspecified diagnosis is not necessarily wrong, it may indicate a documentation deficiency. Unspecified diagnoses indicate the medical record did not have enough information to provide a specific ICD-10-CM code.
As an example, ICD-10-CM S99.919A is for an unspecified injury of unspecified ankle, initial encounter. This code indicates the provider did not document the type of injury or which ankle was injured and may cause a claim delay for review of medical records.
Configuration of Payer Contracts
Billing is often performed without proper consideration to payer contracts. Be aware of all carveouts on your case-rate contracts. Regularly check to ensure payer processing and payments are in line with your contract.
Avoid supervisor billing except when the contract explicitly allows for it. Most payers credential non-physician practitioners (NPPs). When they do, the rendering provider (NPP) should always go on the claim. Failure to comply with this guideline can result in crippling penalties.
In recent years, a practice agreed to a settlement of $4.2 million with the Department of Justice (DOJ) for billing services under a physician while he was traveling internationally. Services were actually performed by NPPs. Another practice paid the DOJ $22.5 million to settle False Claims Act allegations for billing services performed by noncredentialed providers under a credentialed provider.
For private payers, practices run the risk of losing their contract and/or having their payments recouped by the insurance plan.
A side-effect of adopting good front-end practices is improved patient satisfaction and brand loyalty.
