Published on
Urgent message: Although frequently overlooked, routine urinalysis results can serve as an important diagnostic indicator of underlying and potentially life-threatening systemic disease states.
NATALIE SMITH, MS, PA-C
Urinalysis is one of the most common diagnostic tests used in and urgent care medicine. Urinalysis results yield routine clinical information necessary for everyday diagnoses localized to the renal and urologic systems; findings such as pyuria indicative of cystitis or hematuria related to renal calculi are some commonplace examples. However, there are known limitations to urinalysis interpretation for these routine diagnoses, including leukocyte esterase false positives from vaginal contamination (for urinary tract infections [UTIs], a sensitivity of 72%–97% and a specificity of 41%–86%) and nitrite false positives from contamination or exposure of the urine dipstick to air (for UTIs, a nitrite sensitivity of 19%–48% and a specificity of 92%–100%).1 These inconsistencies often lead health-care providers to rely on microscopic urinalysis findings for more objective information or to base their diagnoses on clinical indicators consistent with suspected pathology despite apparently normal urine dipstick findings.
Despite these known limitations, urinalysis should not be overlooked as a potentially powerful diagnostic tool beyond this narrow scope of application. Often it can serve as the first reliable clinical indicator of systemic disease states. It is necessary for urgent care clinicians to properly interpret urinalysis results in their entirety—beyond surface-level findings that merely correlate with the presenting complaint and anticipated diagnosis. Abnormal urinalysis results that are overlooked could be a harbinger for serious systemic pathology.
Case
Medical History
A 65-year-old woman reports that she has had dark urine and dysuria for 1 week. The patient says she hashad recurring UTIs and believes this to be the etiology of her current symptoms, and she immediately requests antibiotic therapy for her condition. The patient has a past medical history of hypertension, hyperthyroidism, and gastroesophageal reflux disease. She has no significant past surgical history or pertinent social history. Her current medications include metoprolol, 12.5 mg orally twice a day; levothyroxine, 50 μg orally once daily; and esomeprazole, 40 mg orally once daily.
Physical Examination
During the provider’s review of systems, the patient says that she has not had any abdominal, back, or flank pain associated with her symptoms. She also says that she has not experienced any constitutional symptoms such as fever, chills, or myalgia. On further questioning, the patient reveals that she has experienced generalized all-over pruritus without evidence of rash; however, she says that she has not had any localized vaginal pruritus, which was part of the chief complaint documented during triage. Findings on review of systems are otherwise negative.
Findings on physical examination are largely unremarkable. During assessment, the patient is seated and is in no acute distress. The patient’s abdomen is soft and nontender. There are normal abdominal bowel sounds in all 4 quadrants, and no rebound or guarding or peritoneal signs are present. No Murphy sign is observed, there is no organomegaly, and there is no bilateral costovertebral angle tenderness. However, the patient does have a slightly icteric appearance, which neither the patient nor accompanying family members are aware of; they appear somewhat bewildered at the suggestion of such a state, reiterating that the patient has a UTI and merely requires antibiotic treatment. The patient’s vital signs are as follows:
- Blood pressure, 146/87 mm Hg
- Pulse, 88 beats/min
- Respiratory rate, 16 breaths/min
- Temperature, 36.8°C
- Oxygen saturation, 98% on room air
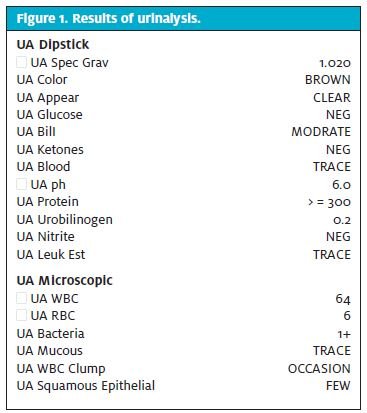
The health-care provider orders urinalysis; findings are shown in Figure 1.
Discussion
Review of this patient’s urinalysis elicited immediate concern. I use the word concern in the sense that only urgent care and emergency department (ED) clinicians can appreciate. This demographic of clinicians is notoriously unimpressed and is generally not overwhelmingly concerned with chronic disease states marked by lack of acuity. A “concerned” ED or urgent care provider typically implies recognition of an immediate or impending threat to life or limb A superficial assessment of the urinalysis findings may lead a clinician to generally agree with the patient’s belief that she does indeed have a UTI and would benefit from antibiotic therapy: 64 white blood cells (WBCs) present on microscopy (with >5 WBCs being significant in women) and 6 red blood cells (RBCs) present on microscopy (with >3 RBCs considered significant) also correlated clinically with the patient’s reports of “dark urine,” dysuria, and urinary frequency. In addition, taking into account the notoriously unreliable nature of negative findings for nitrite and leukocyte esterase (often false negatives), this is not an unreasonable conclusion to make. However, a diagnosis of UTI is not a legitimate explanation for the remainder of the urinalysis findings. The most concerning finding requiring explanation is the problem of bilirubinuria. Absolutes are hard to come by in medicine, but it can be reliably stated that bilirubin in the urine is never normal and often indicates underlying systemic pathology.
Urine does not normally contain detectable amounts of bilirubin.1 Unconjugated bilirubin is not water soluble and therefore by definition cannot pass through the glomerulus. Conjugated bilirubin, however, is water soluble and when present in the urine represents a state of bilirubinuria, yielding a positive bilirubin result on urinalysis. The presence of bilirubinuria directly implicates underlying hepatobiliary disease that must be investigated.1 The only false-positive bilirubinuria results that can occur may be seen if the patient is concomitantly taking the drug phenazopyridine (Pyridium) or the nonsteroidal anti-inflammatory etodolac.1,2 Findings of bilirubinuria should prompt the clinician to elicit a comprehensive medical history will help narrow the differential diagnosis and determine an etiology for the hyperbilirubinemic state.
Questioning should include a thorough medical history involving assessment of any conditions that could be associated with hepatobiliary disease, such as right-sided heart failure, diabetes mellitus and obesity, pregnancy (gallstones), irritable bowel syndrome, celiac disease, and thyroid disease. All prescribed and over-the-counter medications, including vitamins or dietary supplements that the patient is taking, should be recorded because they could be responsible for altering the patient’s liver function. Surgical history (specifically any pertinent abdominal surgical history) and family history for inherited liver or hemolytic disorders should be sought. The social history should seek to obtain any medically pertinent information such as travel to any hepatitis endemic regions and any use of recreational drugs or alcohol that could explain or contribute to hepatic dysfunction in the patient. The most reliable physical examination sign associated with an asymptomatic hyperbilirubinemic state is painless jaundice. Other red flags for chronic liver disease include stigmata of liver disease (spider nevi, palmar erythema, gynecomastia, and caput medusae) and signs of hepatic congestion (abdominal ascites, increased jugular venous pressure, palpable liver enlargement).2 In the setting of unexplained bilirubinuria, a fundamental understanding of bilirubin metabolism is necessary in order to narrow the differential diagnosis.
Understanding Bilirubin Metabolism
What Is It?
Bilirubin is a yellow catabolic byproduct of normal RBC breakdown. After oxidation, it is responsible for urine’s typical yellow appearance and for stool’s typical brown appearance. There are two fractions of bilirubin, conjugated and unconjugated, that comprise the total amount of circulating bilirubin. It is the total bilirubin that is commonly reported on the comprehensive metabolic panel.
Why Is It Important?
A normal serum bilirubin value is simple to remember: typically around 1 mg/dL. Jaundice typically correlates with a serum value of 2.0 mg/dL. Jaundice cannot typically be appreciated on examination at values below this threshold. Remember to check sclera and beneath the tongue, because these areas are affected first.3 Jaundice is often the first (and possibly the only) sign, on physical examination, of liver disease and hyperbilirubinemia, making its detection extremely important in the evaluation and prognosis of those affected.

Understanding Bilirubin Fractions
Conjugated (Direct) Bilirubin
As heme breakdown occurs, bilirubin is sent from the systemic circulation, where it becomes conjugated by molecules of glucuronic acid in liver hepatocytes. Conjugated bilirubin then travels from the liver into the biliary tree as bile, which is stored in the gallbladder and is periodically excreted into the small bowel to aid in digestion. Conjugated bilirubin is by definition the only form of bilirubin capable of being detected on urinalysis. An important aspect of conjugated bilirubin is that it is water soluble, which means it can be excreted in the urine by the glomerulus and is recognized on urinalysis simply as “bilirubin.”
Normally there should be no bilirubin detected on a urine dipstick, and even very small elevations in serum conjugated bilirubin can yield positive results, making this an early and very sensitive and specific marker for underlying pathology. If it is detected, urine bilirubin is a clear indication for further investigation for causes of hyperbilirubinemia.3
Predominant elevation in conjugated (direct) fraction of total bilirubin:
Think backward leakage of conjugated bilirubin (extrahepatic cholestasis) or decreased excretion of conjugated bilirubin (intrahepatic cholestasis).
Extrahepatic cholestasis: This is extrinsic compression and therefore obstruction of the biliary tree, causing backflow of already-processed (conjugated) bilirubin. Differential diagnoses may include tumors caused by malignancy, choledocholithiasis, ascending cholangitis, primary sclerosing cholangitis, pancreatitis, cholangiopathy associated with acquired immunodeficiency syndrome, and biliary strictures, all of which are capable of causing backflow of conjugated bilirubin.3
Intrahepatic cholestasis: This is almost any liver disease or state affecting liver function (hepatitis, cirrhosis, drugs or toxins, sepsis or hypoperfusion).3 Please note that liver disease states can often show mixed conjugated and unconjugated hyperbilirubinemia, depending on the stage and location of liver injury. If injury to the liver is extensive, there will be decreased liver function and therefore decreased conjugating ability, as well as decreased liver uptake of bilirubin, causing increased unconjugated fractions. However, most liver diseases primarily affect canalicular excretion. If injury is localized to the bile canaliculi, there will be a predominant conjugated pattern of hyperbilirubinemia because there is no impairment in liver conjugating ability, but there is impaired excretion of conjugated bilirubin via the bile canaliculi (Figure 2). This is in essence the same concept already described with extrahepatic cholestasis (conjugated hyperbilirubinemia due to obstruction of bile’s normal trek through the biliary tree). It is just an extremely proximal anatomic obstruction, basically at the origin of the biliary tree itself (liver canaliculi). This canalicular obstruction is responsible for sending the conjugated bilirubin back into the systemic circulation and ultimately to the kidney for excretion and detection by urinalysis.3,4
Unconjugated (Indirect) Bilirubin Unconjugated bilirubin is the majority of circulating bilirubin. It has not been processed by the liver (and thus is unconjugated), and it is therefore insoluble and physically cannot be excreted in the urine or appreciated on urinalysis.
Predominant elevation in unconjugated (indirect) fraction of total bilirubin:
Think RBC hemolysis, diminished liver bilirubin uptake, or hepatocyte function
Overproduction:
There is increased unconjugated bilirubin from RBC intravascular or extravascular hemolysis.3,4
Impaired liver uptake or impaired liver conjugating ability:
Potential etiologies include chronic hepatitis, cirrhosis, Wilson disease, Gilbert syndrome, certain antibiotics can inhibit glucuronidation (namely, gentamicin).3,4
Urobilinogen
Urobilinogen is another form of bilirubin also measured on urinalysis that is not to be confused with bilirubin on urinalysis. The take-home point regarding urobilinogen detection on urinalysis is that it is far less useful than bilirubin detection. Normal urine contains small amounts of urobilinogen; it is what makes urine yellow. Urobilinogen levels increase if there is any concomitant liver disease that is nonobstructive (bilirubin has to make it to the gut for it to even exist), but the test is sensitive but not specific for this state, and the level of urobilinogen does not increase in proportion to bilirubin overproduction because the conversion of bilirubin to urobilinogen is actually not directly quantitative.1,3 Urobilinogen is basically just conjugated bilirubin after it has made its trek through the biliary tree and finally into the intestine, where it is enzymatically converted by gut bacteria into colorless urobilinogen. About half of the gut urobilinogen is taken back up into the systemic circulation and can therefore be filtered by the kidney (because it is water soluble). In the kidney, colorless urobilinogen is then oxidized into yellow urobilin, which is technically the final product of bilirubin metabolism that gives urine its typical yellow hue and is seen in healthy individuals.
Urobilinogen that remains in the gut is reduced to brown stercobilin and is responsible for the color of stool.3,5 Hemolytic processes or liver diseases (states that generally produce more bilirubin) of course can lead to increased urine levels of urobilinogen. A complete biliary obstruction or broad-spectrum antibiotics that lead to an alteration in gut flora may result in an absence of urinary urobilinogen.3,5
Given this information, it should be understood that “bilirubin” on urinalysis actually implies conjugated bilirubin: It is impossible to appreciate unconjugated bilirubin on urinalysis because it is not water soluble and therefore cannot pass through the glomerulus.4 What is your differential diagnosis for bilirubinuria? What is your differential diagnosis for bilirubinuria with painless jaundice? What tests do you want to order?
Subsequent Laboratory Tests Ordered for Further
Investigation
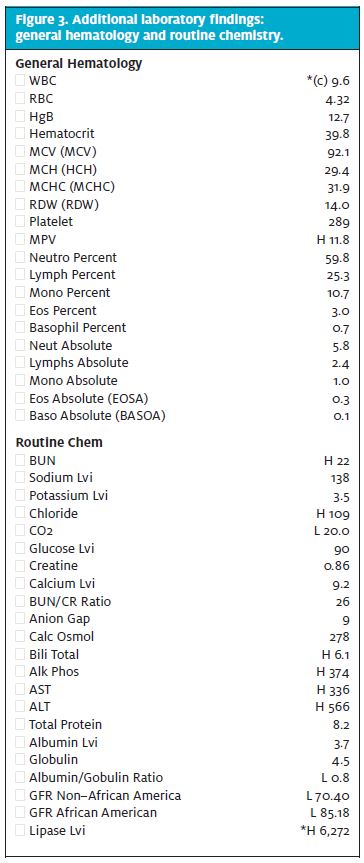
Findings for the additional laboratory tests that were ordered for the patient discussed here are shown in Figure 3.
Other Serum Testing That Could Be Considered
Other serum tests might produce helpful findings.
Prothrombin time or international normalized ratio:
These are markers for the liver’s synthetic ability to manufacture clotting factors. These values are not typically affected in early course of disease because the body has many clotting factor reserves. If prothrombin time is affected, it is a marker of chronicity and severity.2
Prealbumin:
Prealbumin is also a marker of liver synthetic function, and it has a far shorter half-life than albumin (1.9 days vs. 21 days), making it much more clinically useful as a marker for acute alterations in liver synthetic function, because levels fluctuate much more rapidly in response to hepatic injury.2
Basic metabolic and liver function tests (LFTs) instead of a complete metabolic panel (CMP):
The subsequent laboratory investigation for the patient discussed here included an order for a CMP, not an order for a BMP plus LFTs, which would have given the breakdown of conjugated versus unconjugated bilirubin (fractionated bilirubin). Bilirubin fractions in theory seem valuable for classifying the possible etiologies of hyperbilirubinemia. However, this was inherently unnecessary because we know that any bilirubin found in the urine is by definition conjugated bilirubin, which tells us there is a predominant pattern of conjugated hyperbilirubinemia. Positive findings for bilirubin on a urine dipstick test therefore yield the same information that any serum fractionation could, and it is highly accurate.6 Also, although there are appreciated patterns and corresponding differential diagnoses in patients who have hyperbilirubinemia, oftentimes these patterns overlap, making fractionation seemingly less clinically useful.4 There are also widespread technical dilemmas regarding laboratory accuracy when it comes to serum fractionation of the bilirubin concentration.4
Outcome
After inspection of the initial urinalysis findings, your differential diagnosis for this patient should have included causes of conjugated hyperbilirubinemia. Given the asymptomatic presentation, history of present illness, and stable vital signs, your differential should specifically include causes of painless jaundice (and should therefore be narrowed to exclude conditions such as choledo or biliary pain syndromes). Results from subsequent testing (Figure 3) are summarized as follows:
- Dramatic elevation of serum lipase in the absence of abdominal pain, suggesting ongoing secondary pancreatic inflammation (6,272 u/L, in contrast to the normal range of 0–160 u/L)
- A compounded unimpressive pattern of LFT elevation (elevated, but not 20 times the upper limit of normal and dramatically out of proportion to the alkaline phosphatase, as is typically seen in hepatocellular causes such as hepatitis and cirrhosis)
These laboratory findings are most clinically concerning and are consistent with a painless obstructing lesion of the biliary tree. On further questioning, the patient does say that she has had some unwanted weight loss over the past several months and has noted that her stools have become increasingly light in color (acholic) but her urine has become darker. The patient’s symptom of diffuse all-over pruritus in the form of cholestatic pruritus also coincides with a diagnosis of hyperbilirubinemia caused by an obstructing lesion of the biliary tree.7 The mechanism of cholestatic pruritus is poorly understood, but it occurs because of the impaired secretion of bile and is a common symptom seen in certain forms of liver disease.7 After evaluation of these laboratory findings, a computed tomography scan of the patient’s abdomen and pelvis, with intravenous contrast, was ordered to confirm a suspected obstructing carcinoma of the pancreas; results appear in Figure 4.

Clinical Pearls
Urobilinogen represents a normal finding on urinalysis, but bilirubin does not. Do not ignore a positive bilirubin result on urinalysis.
Unexpected bilirubinuria, as evidenced by positive findings for “bilirubin” on urinalysis, may be the first clinical indicator of serious underlying hepatobiliary disease even before clinical jaundice is appreciated on physical examination.
Positive bilirubin on urinalysis indicates a need for further investigation to rule out hepatobiliary disease. This may include a more detailed medical history for explanation of findings or further work-up and definitive laboratory assessment of hepatic function with a CMP or LFTs).
Disposition
The patient was admitted to the hospital for further treatment and therapeutic endoscopic retrograde cholangiopancreatography (ERCP). Admission diagnoses included the following:
- Painless obstructive jaundice
- Pancreatic head mass with concern for pancreatic carcinoma
- Acute obstructive pancreatitis
- Metabolic acidosis
- UTI with alpha-hemolytic streptococci, which is what the patient had actually presented for
The patient underwent ERCP for pancreatic duct cannulation via stent placement and was subsequently referred to the surgical oncology service for further intervention and treatment.
Pancreatic cancer has a 25% survival rate at 1 year, and only 5% at 5 years, which is the lowest survival rate of all major cancers. Men and women are equally affected, and risk factors include advanced age (rarely occurring in those younger than 50 years), smoking, obesity, excessive alcohol consumption, and any family history significant for pancreatic cancer.8 With the exception of advanced age, the patient discussed here demonstrated none of these risk factors; the ultimate key to her diagnosis was accurate interpretation of her urinalysis findings. The majority of these tumors occur in the head of the pancreas, creating an anatomic predisposition toward obstructive biliary syndromes and positive urinalysis findings for bilirubinuria at presentation, as was seen in this patient.
The case discussed here is a vivid reminder that in medicine, clinicians should always consider the worst possible outcome. Even when a patient’s presentation seems unremarkable and routine, the clinician should approach each chief compliant (even alleged vaginal itching) with a high index of suspicion that serious pathology could be present. A case like this one may on the surface seem benign and uncomplicated, but a more meticulous investigation just may reveal a diagnostic wolf in seemingly benign UTI clothing.
References
- Simerville JA, Maxted WC, Pahira JJ. Urinalysis: a comprehensive review. Am Fam Physician. 2005;71:1153–1162.
- Pratt DS, Kaplan MM. Evaluation of abnormal liver-enzyme results in asymptomatic patients. N Engl J Med. 2000;342:1266–1271.
- Zeidner JF, Syndor E. Painless jaundice. Am J Med. 2010;123:601–603.
- Sticova E, Jirsa M. New insights in bilirubin metabolism and their clinical implications. World J Gastroenterol. 2013;19:6398–6407.
- Wolkoff AW. The hyperbilirubinemias. In: Longo DL, Fauci AS, Kasper DL, et al, eds. Harrison’s Principles of Internal Medicine. 18th ed. New York, NY: McGraw-Hill; 2012:2531–2536.
- Pratt DS, Kaplan MM. Jaundice. In: Longo DL, Fauci AS, Kasper DL, et al, eds. Harrison’sPrinciples of Internal Medicine. 18th ed. New York, NY: McGraw-Hill; 2012:324–329.
- Wang H, Yosipovitch G. New insights into the pathophysiology and treatment of chronic itch in patients with end-stage renal disease, chronic liver disease, and lymphoma. Int J Dermatol. 2010;49:1–11.
- Hidalgo M. Pancreatic Cancer. N Engl J Med. 2010;362:1605–1617.