Published on
Urgent message: Epistaxis is a common chief complaint representing a wide spectrum of severity. Key features such as the vital signs, location of the bleeding, and patient history, as well as practice and facility with certain procedures, can assist significantly with patient outcomes and dispositions.
Lindsay Ballard, MD; Stephanie Fernandez, MD; and Joshua Kornegay, MD
Citation: Ballard L, Fernandez S, Kornegay J. Epistaxis: a clinical review. J Urgent Care Med. 2021;15(10):13-18.
Introduction
Epistaxis is a frequent chief complaint in both urgent care and emergency department settings. Approximately 60% of the population will experience some type of nose bleeding in their lives.1,2 Of those, 6% to 10% will seek medical care and 6% may require hospitalization.3-5 One estimate suggests that epistaxis is related to one in 200 ED visits. There is a bimodal distribution in younger (frequently <10 years of age) and older age groups (>50).1,2 In the younger group, digital trauma and lack of humidity (ie, forced heating in the winter) are common causes. In those over the age of 50, deviated septum, anticoagulant use, nasal cannula use, neoplasm, and chemical irritants become more common.1
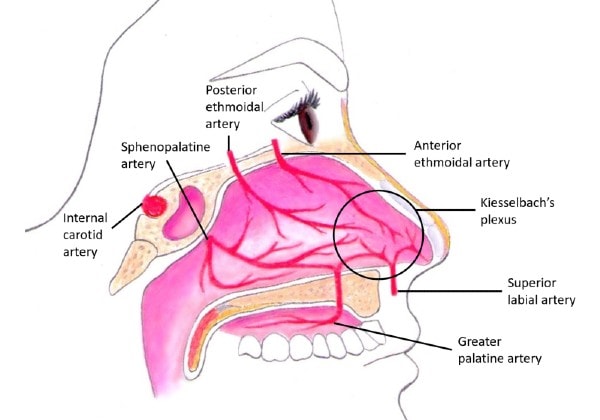
Anatomy plays a large role in management of epistaxis. The vascular system of the nose is extensive and comprised of multiple anastomoses, coming from the internal and external carotid arteries.
Epistaxis is broadly categorized into anterior and posterior, with anterior being much more common, accounting for 80% to 90% cases.4 The Kiesselbach plexus (also called Little’s area) is the most common site of anterior bleeding. It is made up from vessels of the anterior nasal septum, including anterior and posterior ethmoidal arteries, and the internal maxillary artery as well as the sphenopalatine and greater palatine arteries. Posterior bleeding is more likely attributed to the posterior nasal septum and lateral nasal wall, which receives blood from the sphenopalatine artery and branches from the maxillary artery.2
In addition to anterior and posterior, epistaxis is further classified as primary or secondary.
Anterior bleeding is typically more amenable to hemostasis due to smaller vessel size and the ability to compress the vessels, as well as visualize them. Posterior epistaxis can be more difficult to identify given the posterior nature, prolonging management; there is also an increased risk of aspiration.
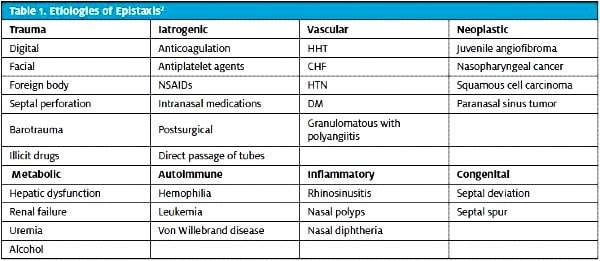
Primary epistaxis is spontaneous or related to environmental factors and accounts for the majority of cases. Secondary epistaxis has an identifiable cause such as trauma and coagulopathy (inherited or pharmaceutical), among other etiologies. The number-one cause of epistaxis is digital trauma.4
Initial patient evaluation should consist of the ABCs (airway, breathing, circulation). Any evidence of instability, including vital-sign abnormalities, airway compromise or respiratory distress, altered mental status, or syncope requires immediate intervention prior to attending to hemostasis of the epistaxis. EMS should be contacted promptly, as these findings necessitate immediate transfer from the urgent care setting to an emergency department.
Initial Treatment
Ideally, the provider will have full PPE, including a face shield as well as a head lamp, for hands-free assessment.After determination of the patient’s stability, the provider can recommend a forward lean and sniffing position to reduce aspiration risk. The patient should initiate 10-20 minutes of uninterrupted firm compression to the anterior third of the nose (just below nasal bones). This is very difficult for many patients and, as such, can be performed with a device, such as a nasal clamp, or enlisting a caregiver to apply force. This is an appropriate time to obtain more information and gather supplies.
To obtain optimal view of the nares, it is recommended that the patient blow their nose to remove any clotted material, followed by immediate application of a topical vasoconstrictor, such as oxymetazoline (commonly known as Afrin). Cotton balls can also be soaked in a vasoconstrictor solution for a more directed topical application. This can be uncomfortable for the patient; topical anesthetic such as lidocaine or LET solution can also be utilized in this setting.
Identification of the source helps direct management strategy and is key to definitive management. There are many useful tools for epistaxis management; see Table 2 for a list of recommended items. If your urgent care center does not have a kit, consider making a kit for ease of use.

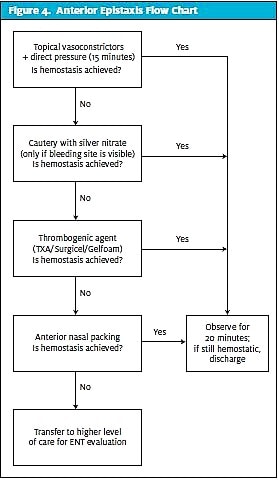
Anterior Epistaxis
If anterior epistaxis is identified on exam, the clinician can proceed with management. Many times, topical vasoconstrictors along with direct compression may induce hemostasis alone. If not, cautery is often considered the next best step.
Cautery is typically performed with a cotton-tipped applicator with silver nitrate on the end. The swab should be applied directly to the identified area of bleeding or around the area and then more circumferentially toward the center. The required chemical reaction cannot occur in the setting of hemorrhage; as such, the field should be clear prior to this technique. A major risk factor of cautery in the anterior nasal septum is perforation of the nasal septum. Sparse cauterization is recommended, and there should never be cautery on bilateral areas of the septum.2 Electrocautery should be reserved for otolaryngologists.1
The next step can be either tranexamic acid (TXA) or thrombogenic foams or anterior packing. TXA is an antifibrinolytic medication and is most commonly administered topically. A TXA-soaked gauze or pledget (500 mg/5 mL) is typically placed in the anterior nares and left in place for approximately 10 minutes. In a Cochrane Review of TXA (utilized orally, intravenously, or topically) for epistaxis as compared to a control (placebo, usual treatment, or usual care with another hemostatic agent) there was a lower rate of rebleeding at 10 days with the use of any kind of TXA vs the control groups. There was no reported significant difference in adverse events, although it is noted one of six trials did not report adverse events. The NNT was reported as 5 for any method of TXA use. Existing evidence suggests there is efficacy for TXA in treating epistaxis.7,8 Thrombogenic foams, such as Surgicel or Gelfoam, can also be applied; these are absorbable and do not require removal.1
Anterior packing is generally considered the last step to anterior epistaxis. There are many brands and types of balloons and nasal tampons for anterior nasal packing. Always consider the possibility of posterior bleeding if direct pressure, vasoconstrictors, cautery, and TXA have not achieved hemostasis. Also note a few contraindications to anterior packing: facial nasal bone fractures, basilar skull fracture, and hemodynamic instability.6 In general, anterior nasal packing functions by providing direct interior pressure to the nasal cavities presumed to have the bleeding vessel. As such, nasal packing is often uncomfortable to place and have in place. Commonly known brands include Merocel and the Rapid Rhino. Additionally, lubricated or antibiotic-soaked gauze is acceptable.
Every type of device has specific directions for usage, although it is generally recommended that they be soaked in petroleum jelly. Anterior nasal packing is left in place for 24–48 hours.2 It is important to tape any drawstrings to the face securely to avoid aspiration. If there are no preformed devices, ribbon gauze packing is an acceptable alternative. There are potential complications to anterior nasal packing, including posterior dislocation (and possible subsequent aspiration), allergic reactions, necrosis of the nasal mucosa, discomfort, and infection such as staphylococcal toxic shock syndrome.
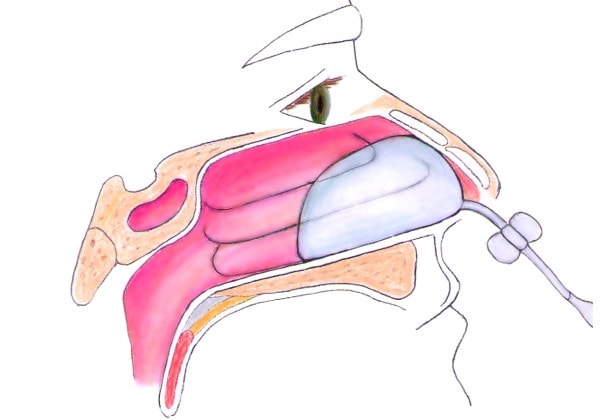
The Rapid Rhino balloon is a preformed balloon that is soaked in water and inserted along the floor of the nasal cavity parallel to the hard palate. Air is then injected with a 20 cc syringe into the balloon, slowly inflating the balloon until tamponade is appreciated. Inflation with water or saline is never recommended due to risk of aspiration with balloon rupture.1 Rapid Rhinos are available in multiple sizes.
The Rhino Rocket is another nasal tampon device, and has an applicator. The sponge is coated with a water-soluble antibiotic ointment and inserted along the floor of the nasal passage, parallel to the hard palate. It should expand within 30 seconds; otherwise, gentle irrigation with a small amount of normal saline can promote additional expansion of the dehydrated tampon. An American randomized controlled trial showed that the Rhino Rocket is easier to insert and less painful for the patient than the Rapid Rhino, but that they are both equally efficacious in achieving hemostasis.9
Many other preformed nasal sponges (such as Merocel, a desiccated polyvinyl acetate sponge that comes in multiple sizes) are also commercially available.
Impregnated ribbon gauze placement is a functional procedure if novel devices are not available, although this is more technically difficult.1 Most manufacturers have both instructive pamphlets with their devices and video instructions online for additional information regarding appropriate placement.
No matter which device is utilized, reassessment is recommended after 10–20 minutes to ensure tamponade has been achieved and the patient is comfortable.
Antibiotic use is controversial in anterior packing. Data from the ENT literature suggest antibiotic use is helpful in postoperative patients to prevent of Staphylococcus infection and associated toxic shock syndrome with residual packing in place.10,11 Antibiotics are often recommended if packing is going to be in place over 48 hours, with preferred classes being cephalosporins, amoxicillin-clavulanate, and trimethoprim sulfamethoxazole.4 Antibiotics are routinely prescribed in posterior packing, however, as well as for patients with valvular heart disease or immunocompromise.2
Regarding ointments: It is recommended that the packing be lubricated as noted above. Additionally, if hemostasis is achieved without packing, it is prudent to prescribe a topical lubricant for the patient for the following week to reduce the risk of re-bleeding. Additionally, nose blowing should be avoided for 7–10 days.
Posterior Epistaxis
Posterior packing typically requires hospital admission with antibiotics. Patients in the urgent care setting identified to have posterior epistaxis should be transferred to an emergency department by EMS for definitive management. While waiting for EMS to arrive, direct pressure can be helpful and the patient should be placed in a position to prevent bleeding from obstructing the airway. Posterior bleeding is more common in adults and should be suspected if there is bilateral bleeding in the nares, significant bleeding visualized in the oropharynx, or if the bleeding cannot be visualized or stopped utilizing the above techniques.
Posterior packing is even more painful and uncomfortable than anterior packing. Proper attention to anesthesia should be given, which may include a nasal block, procedural sedation, or narcotics. Posterior packing is associated with a much higher complication rate including hypoxia, pressure necrosis, infection, and cardiac dysrhythmias. Therefore, posterior nasal packing should be viewed as a temporizing measure while transferring a patient to higher level of care or awaiting ENT expert consultation.1,11
Additional complications include bradycardia, hypotension, arrythmia, infection, sepsis, death, aspiration, and nasal septal necrosis, among others. The patient will likely require admission to the hospital with ENT follow-up.
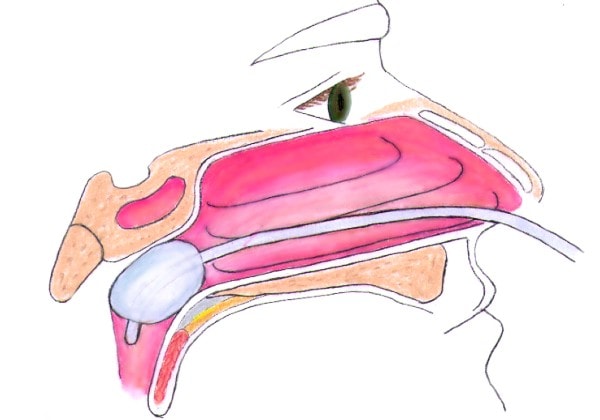
There are commercially available devices for posterior nasal packing, including Rhino Rocket, Epi-Max, and T3100 Epistaxis Catheter. Lastly, a Foley catheter can be used for balloon tamponade. The lubricated catheter is inserted into the nares, inflated with 5 mL to 10 mL of saline, and lodged into the posterior nasal choana. The balloon is then pulled to traction until properly seated and clamped in place. Anterior packing should then be placed into the ipsilateral side.
Special Considerations
Anticoagulants can increase the risk of epistaxis and possibly risk of treatment failure.12 Between 24% and 33% of patients requiring hospitalization for epistaxis are on anticoagulant or antiplatelet medications.4 A retrospective German study showed that anticoagulant use is associated with recurrent bleeding but not more complicated or severe courses of bleeding.13 This may become an area of focus for new approaches to epistaxis management and treatment as the usage of anticoagulants increases. Typically, no changes need to be made to anticoagulant therapy as long as hemostasis is achieved. Reversal or alteration of anticoagulation should be reserved for significant bleeding; however, this should be done in the ED.
Other medications can increase the risk of epistaxis; these include acetylsalicylic acid, NSAIDs, PDE 5 inhibitors, and alcohol.4 Risk factors for admission include antiplatelet or anticoagulant medications, hypertension, diabetes, and posterior bleeding.14
Risk factors for re-bleeding include history of hypertension or heart disease, treatment with gauze packing, and bleeding anywhere other than the nasal septum.15 A small Canadian study showed silver nitrate to have lower re-bleed recurrence odds than petroleum gauze packing and similar to Merocel.12
Hypertension at the time of epistaxis onset has been cited as a possible risk factor or precipitant of epistaxis. There is evidence to suggest correlation, but no strong evidence for causation at this time.16,17
While initial treatment may be the same for patients with known bleeding disorders, recent instrumentation or surgery, or HEENT, those with neoplasms may already have a special treatment plan (such as in hemophilia) or very directed follow-up with their surgeon, for example.
Some patients may require surgical intervention with ENT if hemostasis cannot be otherwise achieved in the outpatient setting. One retrospective Swiss study suggests that surgical intervention is superior to posterior packing when treating posterior epistaxis, with treatment failure rates of 3% vs 38%, respectively.18
Keys to Medical History and Physical Exam
Key components to the medical history include intensity of the bleeding, duration of the bleeding, prior history of epistaxis, trauma, personal or family history of bleeding diathesis, easy bruising, melena, hematochezia, hematemesis, anticoagulant use, or antiplatelet medications, and intranasal drug use.3 OPQRST questions can help elucidate the underlying cause of the epistaxis, particularly in the setting of trauma. Physical exam findings include vital signs, assessing need for resuscitation, localization of the bleeding, and procedural maneuvers to stop bleeding. Additional physical exam findings outside of the HEENT exam, such as cardiovascular and pulmonary, as well as skin, are important components of determining the gravity of the bleeding. If the patient has experienced epistaxis in the past, it can be helpful to know what interventions have achieved hemostasis during previous encounters.
Red Flags
Red flags include tachycardia, hypotension. hemoptysis, hematemesis, suspected airway compromise (such as tachypnea and hypoxemia), adventitious breath sounds like stridor, traumatic injury to the neck or chest, or history of bleeding diathesis, such as hemophilia, hereditary hemorrhagic telangiectasia, or von Willebrand disease. The otherwise healthy young child with an uncomplicated nosebleed presents a different case from an older woman on chronic warfarin therapy, for example.
All patients must be promptly risk-stratified and identified as having requirements for resuscitation and intervention vs having the ability to pinch off their own nose for 5 to 10 minutes.
Diagnostics
In many cases of epistaxis, no laboratory testing or imaging is required. The clinician can consider PT/INR if the patient is taking warfarin or has a known bleeding disorder. Routine use of hemoglobin and hematocrit testing is not recommended, but should be considered if the patient has vital sign abnormalities, ongoing bleeding, history of anemia, or a bleeding diathesis, or if the suspicion for surgical intervention is high. Additional testing such as renal and hepatic function can be obtained in the ED if there is suspicion of large volume blood loss or concomitant gastrointestinal bleed.1
Medical Decision-Making Pearls
The MDM should accurately reflect the patient’s vital signs, along with history of epistaxis, any predisposing factors or comorbidities, and the steps taken to remedy the bleeding. Follow-up instructions and return precautions should be documented clearly, with specific recommendations for the patient. Procedures should be documented appropriately.
Disposition
Further treatment and appropriate follow-up will vary based on the presentation. Specifically in the urgent care setting, if the patient cannot be managed appropriately with initial measures such as direct pressure, vasoconstrictors, and possibly anterior nasal packing or cautery, they should be referred to the ED. Any vital-sign abnormalities such as tachycardia, hypotension, or fever should also warrant consideration for transfer. If the patient is stable to be discharged home, they should be provided with strict return precautions along with home self-care instructions for achieving hemostasis with direct pressure and utilizing the sniffing position for at least 10 minutes, in the event of a re-bleed.
References
- McGinnis HD. Nose and sinuses. In: Tintinalli JE, Ma OJ, Yealy DM, et al, eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide. 9th ed. New York, NY: McGraw-Hill Education; 2020.
- Krulewitz NA, Fix ML. Epistaxis. Emerg Med Clin North Am. 2019;37(1):29-39.
- Tunkel DE, Anne S, Payne SC, et al. Clinical Practice Guideline: nosebleed (epistaxis). Otolaryngol Head Neck Surg. 2020;162(1_suppl):S1-S38.
- Beck R, Sorge M, Schneider A, Dietz A. Current approaches to epistaxis treatment in primary and secondary care. Dtsch Arztebl Int. 2018;115(1-02):12-22.
- Pallin DJ, Chng Y-M, McKay MP, et al. Epidemiology of Epistaxis in u.s. emergency departments, 1992 to 2001. Ann Emerg Med. 2005;46(1):77-81.
- Kravchik L, Pester JM. Anterior Epistaxis nasal pack. StatPearls. Treasure Island (FL) 2020.
- Gottlieb M, Koyfman A, Long B. Tranexamic acid for the treatment of epistaxis. Acad Emerg Med. 2019;26(11):1292-1293.
- Joseph J, Martinez‐Devesa P, Bellorini J, Burton MJ. Tranexamic acid for patients with nasal haemorrhage (epistaxis). Cochrane Database of Systematic Reviews. 2018(12).
- Singer AJ, Blanda M, Cronin K, et al. Comparison of nasal tampons for the treatment of epistaxis in the emergency department: a randomized controlled trial. Ann Emerg Med. 2005;45(2):134-139.
- Cohn B. Are prophylactic antibiotics necessary for anterior nasal packing in epistaxis? Ann Emerg Med. 2015;65(1):109-111.
- Gilman S. Treatment of epistaxis. ACEP Now. 2009;28(26):4-6.
- Newton E, Lasso A, Petrcich W, Kilty SJ. An outcomes analysis of anterior epistaxis management in the emergency department. J Otolaryngol Head Neck Surg. 2016;45(1):24.
- Buchberger AMS, Baumann A, Johnson F, et al. The role of oral anticoagulants in epistaxis. Eur Arch Otorhinolaryngol. 2018;275(8):2035-2043.
- Kallenbach M, Dittberner A, Boeger D, et al. Hospitalization for epistaxis: a population-based healthcare research study in Thuringia, Germany. Eur Arch Otorhinolaryngol. 2020; 277(6):1659-1666.
- Fuji S, Hirai M, Shigehara A, et al. Risk factors for re-bleeding after the treatment of epistaxis. Nihon Jibiinkoka Gakkai Kaiho. 2016;119(8):1117-1126.
- Kim C, Kim C, Chung JH, Shin JH. Is epistaxis associated with high blood pressure and hypertension? Propensity score matching study. Am J Emerg Med. 2020;38(7):1319-1321.
- Min HJ, Kang H, Choi GJ, Kim KS. Association between Hypertension and Epistaxis: Systematic Review and Meta-analysis. Otolaryngol Head Neck Surg. 2017;157(6):921-927.
- Soyka MB, Nikolaou G, Rufibach K, Holzmann D. On the effectiveness of treatment options in epistaxis: an analysis of 678 interventions. Rhinology. 2011;49(4):474-478.
