Published on
Urgent message: Though ear pain is often due to otitis media or externa, it is important to include other diagnoses, some of which could be life-threatening, “can’t miss” causes.
Introduction
Patient complaints of ear pain (otalgia) are seen frequently in the urgent care setting. It can be frustrating for patients and providers when a patient’s ear pain has no obvious cause. Differential diagnoses include several primary and secondary causes of otalgia. (See Table 1.)
Lab values or radiological films are rarely helpful; the best diagnostic tool for ear-pain complaints is a focused physical examination of the patient’s head and neck
| Table 1. Causes to Consider in Diagnosing Ear Pain Complaints in Urgent Care | |
| Otitis media | Tonsillitis |
| Otitis externa | Sinusitis |
| Herpes zoster/Ramsay Hunt syndrome | Nasopharyngeal tumor |
| Mastoiditis | Wegener’s granulomatosis |
| TMJ/bruxism | Temporal arteritis |
| Barotrauma | AMI; angina pectoris; CAD |
| GERD | Thoracic aneurysm |
| Migraines/neuralgia | Foreign body |
| Carotidynia | Cerumen impaction |
| Dental causes | Cellulitis, chondritis, perichondritis |
| Aphthous ulcers | Salivary gland disorder |
| Trigeminal neuralgia | Cholesteatoma, osteoma |
| Mandibular osteomyelitis/tumor | Psychogenic |
| Eagles syndrome | Idiopathic |
| Acoustic neuroma | |
COMMON DIFFERENTIAL DIAGNOSES
Otitis media
General
Acute otitis media (AOM) is an inflammatory and sometimes infectious process of the middle and inner ear which may be suppurative or from a sterile effusion. Chronic serous otitis media (CSOM) is not painful. Noninfectious fluid found in CSOM can persist in the middle ear for up to 12 weeks.
The peak incidence of AOM occurs in children under the age of 2 and is more common in boys than in girls. By age 6, 90% of children will have had at least one ear infection. Viral infections are the cause of 70% of these ear infections.1,2
The most common viral causes are:
- Respiratory syncytial virus
- Rhinovirus
- Coronavirus
- Influenza
- Parainfluenza
The most common bacterial infections are:
- Streptococcus pneumonia
- Haemophilus influenza
- Moraxella catarrhalis
- Gram-negative enteric bacteria
- Staphylococcus aureus
Mixed viral and bacterial infections occur frequently.3 The incidence of mixed infections reported in the literature varies from 20% to 60%.4
Ear infections occur most frequently in the winter months. Risk factors include bottle-feeding, exposure to second-hand smoke, attending daycare, allergies, family history, and craniofacial abnormalities. The patients may describe widely different patterns of onset, pain, aggravating and relieving factors.
History
Include previous ear infections, ear surgeries, and environmental allergies and treatment in your patient’s history. Ask your patient about any recent travel, flying, or trauma. A pediatric history should include birth, delivery, immunizations, current development, secondhand smoke exposure, allergies, and daycare attendance.
If your patient has fluid in their middle or inner ear they will have decreased, muffled, or absent hearing; this can be assessed with finger rub and whisper tests. Positive Weber and Rinne tests will specifically indicate a conductive hearing loss if there is fluid present in your patient’s middle or inner ear.
Exam
Upon otoscopic examination, air-fluid levels may be present with or without purulence and erythema. observation of drainage in the ear canal is indicative of acute suppurative otitis media. Submandibular and deep cervical chain nodes are usually the first to become swollen in patients with AOM; however, palpation of the head and neck may or may not demonstrate any swollen lymph nodes. Pneumatic otoscopy is 70%–90% sensitive and specific for determining the presence of middle ear effusion.5 In most cases, visualizing a bulging, erythematous tympanic membrane is sufficient for diagnosis.5 Cloudy tympanic membrane is 90.8% sensitive, 91.7% specific.6 Bulging TM is 61.2% specific, 96.9% sensitive. Ear rubbing is 42% specific, 87% sensitive.
AOM is not particularly common in adults. According to the most recent American Association of Pediatrics (AAP), oral antibiotics are recommended for AOM (bilateral or unilateral) in children 6 months and older with severe signs or symptoms. Severe AOM is defined as moderate pain for 48 hours and fever greater than 102.2⁰F. Antibiotic therapy should be used for bilateral AOM in children 6 months through 23 months of age without severe signs or symptoms. If AOM is unilateral, close follow-up is appropriate. Monitoring with close follow-up is recommended for patients with less than severe symptoms who are greater than 12 months old. Close follow-up can be accomplished via phone call or office visit. Resolution of acute pain and purulence is typically seen within 48 hours of onset without antibiotic therapy.2,7
Antibiotic therapy is summarized in Table 2.2,3,7,8
| Table 2. Antibiotic Recommendations and Dosing | |||
| Drug | Dose | Frequency | |
| 1st line therapy | Amoxicillin | Children: 90 mg/Kg/day total | 3 times daily |
| Adults: 875 mg | 2 times daily | ||
| Pt treated with antibiotic in past 30 days | Augmentin | Children: 90 mg/Kg/day total | 3 times daily |
| Adults: 875 mg | 2 times daily | ||
| PCN allergy | Azithromycin | Children: 10 mg/kg 1st dose, then 5 mg/kg doses 2 thru 5 | Once daily |
| Adults: 500 mg 1st dose, then 250 mg doses 2 thru 5 | Once daily | ||
| Alternatives | Cefdinir | Children: 14 mg/kg/day | Once daily |
| Adults: 300mg | 2 times daily | ||
| Cefuroxime | Children: 30 mg/kg/day | 2 times daily | |
| Adults: 250 to 500 mg | 2 times daily | ||
| Cefpodoxime | Children: 10 mg/kg/day | 2 times daily | |
| Adults: 100 to 400 mg | 2 times daily | ||
| Ceftriaxone | Children: 50 mg/kg (max 1 gram) IM | Once daily | |
| Adults: 1 to 2 g IM | Once daily | ||
| *Children <2 years are treated for 5-7 days. Children >2 years are treated for 5-7 days. Adults are treated for 10 days. | |||
If an individual has myringotomy tubes or a perforated eardrum, use drops. Do not irrigate. You will know if patients with tubes have an ear infection because their tubes will drain. Insert 2-3 drops in the affected ear three times daily; ear canals are small and cannot hold more liquid than 2-3 drops. Table 3 gives an overview of antibiotic ear drops.2,3,7,8
| Table 3. Antibiotic Eardrops: An Overview | ||
| Bacterial | ||
| 2% acetic acid | Inexpensive | 2-3 drops in affected ear 3 times daily. Use for 7 to 10 days |
| Neomycin otic | Contact dermatitis develops in 15% of patients | |
| Polymixin B | Avoids neomycin sensitivity
Ineffective against Staph and Gram + bacteria |
|
| Aminoglycosides | Ototoxicity risk | |
| Fluroquinolones | Well tolerated
Expensive Risk of ATB resistance if used frequently |
|
| Combination ATB with steroids | Can be very expensive | |
| Fungal | ||
| 2% acetic acid | Cheap | 2-3 drops in affected ear 3 times daily. Use until infection is resolved |
| Clotrimazole solution | Works on both candida and aspergillus | |
| Itraconazole | Resistant aspergillus may require oral therapy | |
ATB, antibiotic
Otitis Externa
General
Otitis externa (swimmer’s ear) is an infection of the outer ear canal. It is a very painful condition and can be associated with radiation of pain, pruritus, hearing loss, or drainage. Patients often complain of a feeling of fullness in the affected ear. Onset of otitis externa may be rapid or slow and may, or may not, be associated with a fever.9 Pain may be worse with motion or manipulation of the ear.
Otitis externa is caused by an infectious pathogen entering the skin of ear canal, often due to microabrasions from Q-tips, ear buds, or hearing aids.
History
Inquire about swimming and other potential sources of moisture, such as earplugs, eczema, psoriasis, dermatitis, or acne. The most common bacterial pathogens are Pseudomonas aeruginosa and Staphylococcus aureus. Ten percent of these infections are fungal, typically aspergillus or candida.3 Otitis externa is often caused by more than one pathogen.3
Exam
Visual inspection may reveal redness, swelling, or scaling of the external ear. There may be visible drainage (otorrhea). Lymphadenopathy may be palpable at the base of the ear. Hearing will be decreased in the affected ear. Otoscopic exam may be difficult if there is drainage. If there is no drainage, mucopurulent debris is seen in the ear canal. Fungal debris may be fluffy white (Candida) or dark in color (Aspergillus).
Eczema and other skin conditions can be particularly troublesome for patients. Dry skin around the ear can cause itching. Controlling the eczema is necessary to prevent otitis externa from developing. Steroid creams such as triamcinolone can be used up to 3 times daily. A referral to dermatology or otolaryngology for these patients should be considered.
Management
Otitis externa treatment starts with cleaning of the ear canal. The underlying skin is usually very macerated and inflamed; irrigation with water can be performed after a perforated eardrum is excluded.
An ear wick may be inserted if the canal is swollen. Ear wicks should fall out within 24-48 hours. Patients should be seen 2-3 days after insertion of an ear wick to ensure the ear wick fell out and the patient’s infection is resolving. Severe pain out of proportion to physical exam findings may be from malignant otitis externa; emergent referral is recommended. For patients in whom a wick is poorly tolerated, or cases where the canal is blocked, oral antibiotics may be needed.
Patients should be strongly encouraged to refrain from inserting anything into the ear for the purpose of cleaning the ear. Swimmers should consider getting custom earplugs made by an audiologist.
Ramsay Hunt Syndrome
General
Ramsay Hunt syndrome is caused by the varicella zoster virus in patients who have previously had chickenpox; the virus lays dormant until a shingles outbreak occurs. Ramsay Hunt syndrome is characterized by a unilateral vesicular facial rash, which involves portions of the patient’s ear, mouth, neck, and scalp. Cardinal signs also include paralysis of facial nerves on the affected side and a loss of taste on the anterior two-thirds of their tongue (Figure 1). Either the rash or the facial paralysis may come first. Symptoms can last for several weeks. Symptoms may be permanent. Pain characteristics, aggravating factors, and relieving factors can vary widely. Symptoms are persistent and may include tinnitus and/or dizziness.
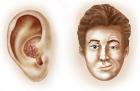
Figure 1. Ramsay Hunt Syndrome
History
Obtain a history of childhood illnesses and vaccinations. The patient may have a recent history of shingles or similar rashes. Ask if there is any previous history of vertigo, hearing loss, or facial paralysis. Also, inquire about new medications (specifically immunosuppressive therapies and steroids), history of stroke, blood clots, or vascular disease.
Exam
Visual inspection will demonstrate a vesicular rash on the external ear, face, and scalp. Look for signs of infection to the eye. Complete a neurological exam. Have your patient raise their eyebrows, smile showing their teeth, and stick out their tongue. Facial weakness on one side will be noticeable. Whisper and finger rub testing will reveal diminished hearing on the affected side. Weber and Rinne will indicate sensorineural hearing loss. You may observe vesicles inside the ear canal upon otoscopic examination.
Management
Treatment is most effective if started within the first 72 hours after the rash develops. Antiviral medications have demonstrated a decrease in the duration of illness and reduced incidence of post herpetic neuralgia. Patients over the age of 50 years have the largest benefit from treatment. Valacyclovir 1,000 mg by mouth three times daily for 5 to 7 days is the first-line therapy, but acyclovir and famciclovir may also be used). A prednisone taper has been shown to decrease pain in patients over 50 years of age.10 Cool, wet compresses can help with itching and painful rash. Moisturizing eye drops should be used during the day. Eye lubricants may be needed at night. The affected eye should be taped shut to prevent injury.
Mastoiditis
General
Mastoiditis is a potentially life-threatening infection of the mastoid air cells behind the ear. This infection is caused by Streptococcus pneumonia, Streptococcus pyogenes, Staphylococcus aureus, Haemophilus influenza, or Moraxella catarrhalis.11 Symptoms are present 2-6 days after the onset of acute otitis media. Mastoiditis is more prevalent in children but can also occur in adults.
Onset of mastoiditis is gradual and usually follows an episode of otitis media or upper respiratory infection. Pain is severe, constant, and isolated to the affected ear. It may be described as sharp, dull, or aching. Pain may persist for days or even weeks. Aggravating factors typically include palpation, chewing, swallowing, and walking.
History
The medical history should include an inquiry about antibiotic use within the past 30 days. Obtain a history of hearing loss. Inquire whether the patient has a history of diabetes, stroke, blood clots, or myringotomy tubes. Consider ruling out blood clots in the brain if there have been any changes in vision or headache.
Exam
On examination, the patient will have retro auricular pain and tenderness over the mastoid. Erythema, warmth, and swelling behind the auricle of the affected ear should raise a strong suspicion for mastoiditis.
Testing
A CT scan with and without contrast of the temporal bones should be ordered if mastoiditis is suspected based on exam findings. Emergent referral to ENT or transfer to the ED is recommended.
Immediate referral to ENT is needed if mastoiditis is present. These patients frequently require hospitalization and close monitoring.
Temporal Mandibular Joint Dysfunction
Temporal mandibular joint (TMJ) dysfunction includes pain in the muscles of mastication or the TMJ joint. It is most common in women between the ages 20 and 40 years of age. It is the second most common cause of orofacial pain.12,13 Trismus, spasms, myositis inflammation, trauma (dislocation/fracture), degenerative arthritis, or infection can all cause TMJ pain.
Past medical history may include recent dental work, grinding teeth (bruxism), braces, baby teeth falling out, or eruption of adult teeth. Aggravating factors can include chewing, yawning, jaw clenching, and walking. The pain is often characterized as dull, achy, poorly localized, intermittent, and unilateral.
Physical examination includes special attention to the temporalis, buccinators, and zygomaticus muscles. Make sure to palpate the masseter muscle at the back of the jaw. It is located behind the teeth, and it is necessary to palpate in the mouth with a gloved hand. This muscle opens and closes the jaw. Sometimes it is the only location patients will feel pain on palpation. The masseter muscle forms the front wall to the ear and is often the reason pain is felt in the ear. Have the patient open and close their mouth while palpating the TMJ joint. Feel for popping, clicking, or dislocation of the joint with opening and closing of the mandible.
Treatments include: no gum chewing, soft diet, NSAIDs, and alternating ice and heat to the affected area for 20 minutes, three times daily. Muscle relaxers may be of benefit for some patients with severe pain.13 Cyclobenzaprine 10 mg up to three times a day can be prescribed. In older patients or those with contraindications to cyclobenzaprine; baclofen 10 mg up to three times daily may be a better alternative.14,15 Referral to a dentist that treats bruxism may be necessary for some patients.
Barotrauma
Barotrauma is caused by significant atmospheric pressure changes and results in damage to the tympanic membrane and other ear tissues. Barotrauma usually occurs during diving or flying. It can occur when a patient is slapped with an open hand. Patients with congestion prior to flying can be susceptible to barotrauma. It is common for patients to report allergies or nasal congestion prior to the incident giving rise to their barotrauma diagnosis. A history of chronic ear infections or myringotomy tubes may predispose a patient to barotrauma injury. Physical examination will reveal a visible perforation or fluid or blood in the canal.
Management
Symptomatic management includes healing with time; antibiotics, steroids and decongestants have not been shown to improve healing. Nonemergent surgery may be necessary for severe injuries.
Prevention
Patients with nasal congestion may use a nasal decongestant—2 squirts in each nostril prophylactically when traveling on a plane. This will open the Eustachian tubes and help equalize middle ear pressures. A steroid nasal inhaler, two squirts in each nostril, twice daily for two weeks prior to flying will also help to shrink the turbinates and the lining of the sinus cavities.16 This aids in maintaining normal inner ear pressures. Likewise, frequent swallowing also helps equalize inner ear pressure. It can be helpful for patients susceptible to barotrauma to have water, chewing gum, and hard candy available when flying.
Gastroesophageal Reflux Disorder
HPI
Gastroesophageal reflux can cause a multitude of symptoms, including otalgia, globus sensation (feeling of a lump in the throat), heartburn, chest pain, radiating pain, hoarseness, throat clearing, nausea, and regurgitation of food. The first symptoms for them may be globus sensation or ear complaints.17 Past medical history may include heartburn or treatment for reflux. Physical examination will be unremarkable. This diagnosis is made based on history.
Discuss dietary modifications such as limiting caffeine, nicotine, and alcohol. Other things to avoid are whole milk products, chocolate, peppermint, cinnamon, tomatoes, and anything that aggravates symptoms. The initial treatment is H2 blockers or proton pump inhibitors (PPIs). Patient should be encouraged to take these medications 30 minutes prior to eating on an empty stomach.8 Patients need referral to the emergency room if they are having trouble swallowing or breathing. Referral can also be made to otolaryngology to confirm the diagnosis.
Other Potential Diagnoses
Other diagnoses to consider were listed in Table 1. Most are caused by an insult or aggravation to a cranial nerve. Some causes of otalgia are simple, such as embedded foreign bodies, cerumen impaction, or cellulitis. Some causes of otalgia can be life-threatening, such as acute myocardial infarction and thoracic aneurysm.18 Otalgia is frequently caused by otitis media; nevertheless, the provider should consider the causes enumerated in Table 1 when formulating a differential diagnosis during an atypical examination.
Conclusion
Complaints of otalgia are frequent in the urgent care setting, with patients often believing they have an ear infection that warrants a prescription for an antibiotic prescription. Consideration of an expanded differential may lead the provider to discover an alternative diagnosis. Approach each patient with an open mind and look for the clues that will help formulate an accurate diagnosis.
Citation: Phelps B, Phelps K. Ear pain mimics: it’s not all about otitis media. J Urgent Care Med. December 2019. Available at: https://www.jucm.com/ear-pain-mimics-its-not-all-about-otitis-media/.
References
- Earwood JS, Rogers TS, Rathjan NA. Ear pain: diagnosing common and uncommon causes. Am Fam Physician. 2018;97(1):20-27.
- Rosenfeld R, Shin J, Schwartz S, et al. Clinical Practice Guideline: Otitis Media with Effusion (Update). Otolaryngol Head Neck Surg. 2016;154(2):201-214.
- Uphold CR, Graham MV, eds. Clinical Guidelines in Family Practice. Gainesville, FL: Barmarrae Books, Inc.; 2013.
- Bakletz L. Immunopathogenesis of polymicrobial otitis media. J Leukocyte Biol. 2010;87:213-222.
- Burrows HL, Blackwood RA, Cooke JM, et al. Otitis Media. University of Michigan. Available at: http://www.med.umich.edu/1info/FHP/practiceguides/om/OM.pdf. Accessed November 11, 2019.
- Rothman R, Owens T, Simel D. Does this child have acute otitis media? JAMA. 2003;290(12): 1633-1640.
- Lieberthal AS, Carroll AE, Chonmaitree T, et al. The diagnosis and management of acute otitis media. Pediatrics, 2013;131(3):e964-e999.
- Gilbert DN, Eliopoulos GM, Chambers HF, eds. The Sanford Guide To Antimicrobial Therapy. 47th ed. Sperryville, VA: Antimicrobial Therapy, Inc.; 2017.
- Schafer P, Baugh R. Acute otitis externa: an update. Am Fam Physician, 2012;6(11):1055-1061.
- Ryu EW, Lee HY, Lee SY, et al. Clinical manifestations and prognosis of patients with Ramsay Hunt syndrome. Am J Otolaryngol. 2012;33(3):313-318.
- Wald ER. Acute mastoiditis in children: clinical features and diagnosis. In: UpToDate, Edwards MS, Messner AH, eds. Waltham, MA, 2018.
- Bueno C, Pereira D, Pattussi M, et al. Gender rdifferences in temporomandibular disorders in adult populational studies: a systematic review and meta‐analysis. J Oral Rehabil. 2018;45(9):720-729.
- Mehta RN. Temporomandibular disorders in adults. In: UpToDate, Kunins L, ed. Waltham, MA, 2019.
- Food and Drug Administration. Cyclobenzapine: Prescribing Information. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/021777s017lbl.pdf. Accessed November 7, 2019.
- Food and Drug Administration. Baclofen: Prescribing Information. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/208193s000lbl.pdf. Accessed November 7, 2019.
- Chang C. Correct use of nasal sprays for eustacian tube dysfunction. Faquier ENT Constultants; September 13, 2018. Available at: https://www.fauquierent.net/etd2.htm. Accessed November 7, 2019.
- Flint P. Throat disorders. In: Goldman L, Schafer A, eds. Goldman-Cecil Medicine. Philadelphia, PA; Elsevier; 2020: 2565-2571.
- Amirhaeri S, Spencer D. Myocardial infarction with unusual presentation of otalgia: a case report. Int J Emerg Med. 2010;3(4):459-460.

Beth Phelps, DNP, ACNP, CNP
