Published on
Urgent message: Effective management of head lacerations starts with hemorrhage control but also requires an understanding of appropriate use of anesthesia, the possibility of closed head or nerve injury, and vigilance for non-accidental trauma.
Clayton Josephy, MD, Samuel M. Keim, MD, MS, and Paper Rosen, MD
Introduction
Laceration repair is a common and important responsibility of physicians in the emergency and urgent care settings. A recent review of national trends in ED visits revealed that approximately 8% of presentations are for lacerations, with approximately one third of those involving structures of the head.1
Management and repair of soft tissue injuries to visible areas of the head tend to be especially important to the patient due to cosmetic considerations. Wounds that involve borders, margins, or multiple anatomic tissue layers have significant cosmetic and functional implications.
General Approach
As is the case with emergent medical assessment, evaluation of a head laceration begins with the “ABCs.” Lacerations of the head, especially those involving the oral or nasopharynx areas, can produce large amounts of hemorrhage, possibly resulting in airway compromise. Often, hemorrhage control (the primary focus of this article) can be achieved by direct pressure on the bleeding site. Blind clamping of vessels should be avoided, as in any other part of the body.
Following hemorrhage control, exploration of a wound is facilitated by anesthetizing the injury. In some patients, systemic analgesia will be indicated and should be administered without undue delay. Topical anesthesia is particularly helpful in children, where needle infiltration may cause significant anxiety and discomfort.
2
With multiple or very large lacerations, it is often useful to anesthetize and repair one wound or one portion of the wound at a time. This will prevent overdose of local anesthesia, or having t wear off before the repair is carried out.
The maximum lidocaine infiltration without epinephrine should be 4.5 mg/kg (not to exceed 300 mg); for lidocaine with epinephrine, it should be 7 mg/kg. Toxicity thresholds, however, are variable among individuals, with some experiencing effects at relatively low doses. Vascularity of the injection site and speed of injection also play a role.3
Copious irrigation with sterile normal saline under pressure remains a common practice, which we recommend (although recent literature suggests that tap water is an acceptable alternative4).
Many repairs can be improved by careful local excision and debridement of devitalized or necrotic tissue. If the resultant wound will require moving a flap of tissue for coverage, or the placement of a skin graft, it is prudent to consult a plastic surgeon.
Generally, there is no role for prophylactic antibiotics in the management of head lacerations. The face, in particular has a rich vascular supply and, therefore, a rate of infection lower than tissues with poorer blood supply.
On the head, wounds can safely be closed up to 12 hours after the laceration was sustained. If the wound is considerably older than 12 hours or if there is clear contamination of the wound (e.g., soil, asphalt, pus) then a delayed primary closure should be considered. This means thorough cleansing, moist dressing the wound, repeat cleaning daily, and closing the wound on day 3 or 4 when it is clear that it is not infected.
Culturing and antibiotics are indicated if the wound appears infected during this management. If the wound is infected or still contaminated after this period, it can be allowed to granulate closed without a formal repair, and then in four to six weeks, when all infection has subsided, it can be excised and closed primarily. This will of course leave a worse cosmetic scar, but it will still be superior to closing the dirty wound and having an abscess form at the site.5
The key to the best cosmesis of the repair is optimal approximation and timely removal of sutures. Typically, this requires a layered closure. If only the epithelial layer is closed on wounds that fully penetrate into subcutaneous tissue, and sutures removed before tissue strength regained, the final scar will resemble the width of the wound before it is closed.
The dermis should be closed with a suture material that will hold for 21 days. This can be achieved with both absorbable and non-absorbable material. For example, the dermis can be closed with monofilament nylon, but this can leave a palpable mass of suture material under the skin and possible discomfort for the patient. It can also be closed with catgut, though this material is weaker and produces an intense inflammatory reaction.6
Suturing needles come in different sizes and types, with the 3/8 arc, reverse-cutting needle used commonly for superficial laceration repair. In general, the needle size is chosen by considering how deep and wide (they should be roughly equal) a suturing “bite” you wish to make.
The epithelium can be closed with a paper wound closure system (e.g., Steri-strips), glue, or sutures. Most physicians prefer very small monofilament nylon for the face (5-0 and 6-0) and larger for the scalp (2-0 and 3-0). Sutures in the facial epithelium should be removed in three to five days for optimal cosmesis. The wound should be kept covered and dry for 24 hours and inspected at 48 hours for evidence of infection. Some physicians like to apply a layer of antibiotic ointment or petroleum jelly as a barrier and to keep the scab from becoming enmeshed with the sutures. Wound infection with careful primary closure on the head should be around 1%.
6
Cosmetic repair is less important for the scalp unless it is bald. Closure here is facilitated by shaving a small area of scalp hair, although this is not necessary for protection against infection. A single layer closure will suffice, with a running monofilament nylon suture of 2-0 or 3-0 gauge. This should be removed in seven to 10 days. Analgesia should not be delayed as part of the management of lacerations, although most wound pain will be adequately managed with an adequate instillation of local anesthesia. The circumstances of the mechanism of injury is sometimes difficult to evaluate, and non-accidental trauma should be considered.6-10
Tetanus status be reviewed (and documented) as part of every wound evaluation. Tetanus immunity wanes over time at an unpredictable rate, and screening is especially important in the elderly patient.11 Current recommendations are that anyone with uncertain tetanus status in the last five years should receive a booster, and children under 7-years-old should receive DTaP unless contraindicated (Table 1).11-14
Table 1. Guidelines for Tetanus Prophylaxis in Routine Wound Management |
||||
| Tetanus | Clean, minor wounds | All other wounds* | ||
| No vaccination history | Td+ | TIG | Td+ | TIG |
| < 3 doses or unknown status | Yes | No | Yes | Yes |
3 or more doses:
|
NoŦ NoŦ Yes |
No No No |
No Yes Yes |
Noᵟ Noᵟ Noᵟ |
| * Wounds such as, but not limited to, those contaminated with dirt, feces, soil, and saliva; puncture wounds; avulsions; and wounds resulting from missiles, crushing, burns, or frostbite. + For children younger than 7 years, DTaP (DT, if pertussis vaccine is contraindicated) is preferred to tetanus toxoid alone. For patients 7 years or older, Td is preferred to tetanus toxoid alone.Ŧ If only 3 doses of fluid toxoid have been received, then a fourth dose of toxoid, preferably an adsorbed toxoid, should be given. ᵟ Yes, if HIV-infected, regardless of immunization history. Td= tetanus-diphtheria toxoids (adult type); TIG= tetanus immune globin; DTap= diphtheria and tetanus toxoids with acellular pertussis vaccine; DT= diphtheria and tetanus toxoids, adsorbed, pediatric strength. Source: Epidemiology & Prevention of Vaccine Preventable Diseases. 8th Ed; 2004. |
||||
Specific Anatomic Considerations
Scalp
The scalp laceration may produce enough hemorrhage to lead to hypovolemic shock. While this is more common in children, it can occur in adults, often in an alcohol-intoxicated patient who is bleeding from a scalp wound while “sleeping it off.”
Scalp bleeders are hard to control, but control is useful in order to complete the rest of the evaluation. Two suggested methods are to either place a series of Raney clips that compress the bleeding vessel against the scalp or to quickly close the laceration with a running 2-0 Mersilene suture. After the evaluation of the patient is complete, either of these modalities can be removed and a more cosmetic repair achieved.
Wounds caused by significant force should promote concern for skull fracture or intracranial injury. This will likely require CT scan and evaluation for possible cervical spine injury
Lips
Lip lacerations are a technical challenge, since even minute deviations form anatomical alignment can result in unsightly scar formation. The vermillion border must be meticulously repaired if involved. Some find that marking the border edges with a tuberculin-syringe injection of methylene blue aids this.
Even a malalignment of 1 mm will be apparent. If the clinician in unsure that his training and experience has prepared him for this procedure, referral is the best option.
Anesthesia can be obtained using topical lidocaine-adrenaline-tetracaine. Regional anesthesia of the ipsilateral mental nerve block will cover half of the lower lip; similarly, an infraorbital nerve block will do the same for the upper lip (Figure 1).15 Generally, nerve blocks are preferable to local infiltration when possible to avoid distortion of the anatomy.

Lacerations involving only the intraoral buccal mucosa frequently do not require closure unless the defect is large enough to trap food particles, due to the inherent vascularity and rapid epithelialization of mucosal tissue. Lacerations that exceed 1 cm in length should be closed using 4-0 absorbable suture with either interrupted, mattress, or running sutures.6 Full thickness buccal lacerations require a three-layer closure to re-establish integrity of oral form and functional competency. Many ED and urgent care physicians will choose to refer these to a plastic or oral surgeon. Some oral surgeons recommend prophylactic antibiotics if the mucosa is penetrated.
Tongue
Typically, lacerations of the tongue occur from falls, penetrating trauma, or during seizures from bites. The majority of tongue lacerations need no closure. Indications for closure include persistent bleeding and major anatomic deformity (especially edges and tip). Partial amputations need referral to ENT or oral surgery.6
Anesthesia of the tongue is difficult to achieve due to its very vascular structure; in addition, local anesthesia wears off quickly. If the laceration involves only one side of the tongue, a lingual block may be used. A bite block is useful and prudent to maintain oral patency, and to protect the physician while repairing the tongue laceration. After adequate anesthesia is obtained, a towel clamp can be applied to the distal tip of the tongue for traction.
The wound should be approximated with widely spaced sutures using deep throws to close the entire wound in one layer. Multiple layer closure is unnecessary. Patients should be given analgesia, and instructed to swish and spit with oral antiseptic mouth wash twice a day following discharge. Depending upon the suture material chosen, the sutures can either fall out on their own or be removed within a week.
Eyelid
Simple lacerations to the eyelid can be managed in the urgent care center, provided they are superficial and do not include the lid margin (Table 2 identifies presentations that may warrant immediate referral). A thorough examination of the globe is warranted to rule out possible injury.
Simple lacerations to the upper eyelid should be repaired using fine nonabsorbable suture material. Don’t use tissue adhesive near the eye. Anesthesia should include careful soft tissue infiltration. The dermis is a very thin layer on the eyelid, but dermal approximation is particularly important. If the physician has no experience with the use of very fine sutures, then referral to the ophthalmologist or plastic surgeon is prudent.
If the lid margin or the under surface of the eyelid (the corneal side) is involved, the patient should be referred to the ophthalmologist. This also should be done for those lacerations near the nasal margin of the lid that might or do involve the lacrimal duct. When in doubt, assume the duct is involved and refer the patient.
Table 2. Emergent Eyelid Referrals |
|
Ear
The anatomy of the ear is composed of cartilaginous framework covered by a thin layer of perichondrium and very thin layer of subcutaneous tissue and skin, making repair quite difficult. The innervation of the ear is complicated and supply is from branches of the trigeminal nerve, the facial nerve, the cervical plexus via the auricular nerve, and branches of the vagus nerve. Lacerations of the ear are often complex.
Because of the frail anatomy and tenuous vascular supply to underlying structures, the auricle (external ear or pinna) is prone to complications, including avascular necrosis of cartilage, infection, abscess, and hematoma formation. Failure to drain a pinna hematoma leads to failure of the perichondrium to adhere to the underlying cartilage. This, in turn, leads to the inflammatory fibrosis calcification known as “cauliflower ear.”
Wound management of ear lacerations should include an assessment of the tympanic membrane. A hemotympanum indicates the presence of a basilar skull fracture. Otorrhea is hard to detect, and should be looked for when there is a hemotympanum.
Persistent oozing in the ear canal may, in fact, be otorrhea rather than a simple laceration of the ear canal. Application of a piece of filter paper or ordinary tissue paper may demonstrate a layering of the fluid that represents otorrhea. If either a hemotympanum or otorrhea is found, the patient will need a head CT scan, and should have a neurosurgical consultation. Prophylactic antibiotics are not helpful, and should not be used.
Since the seventh and eighth cranial nerves run near the ear, any laceration of the ear is an indication to test the function of these two nerves. A partial 7th nerve injury may include loss of taste over the anterior 2/3 of the tongue. An alcohol swab can be used to test taste if there are no other substances conveniently available.
Obtaining anesthesia of the auricle is done by a number of methods. Local wound infiltration is best avoided due to the thin nature of the damaged tissue and potential of further dissection of the perichondrium form the cartilage.
The great auricular nerve can be blocked regionally by infiltrating along the anterior surface of the sternocleidomastoid. Alternatively, regionally blocking the inferior supply of the auricle can be done by infiltrating inferior to the auricle itself. It is important to include the pre-tragal area.
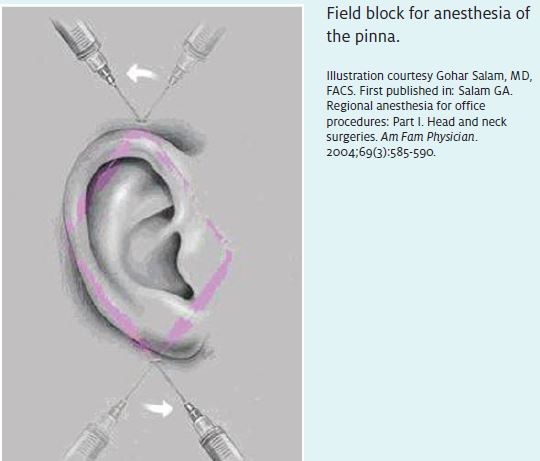
The superior innervation is supplied by the V3 blocked of the trigeminal nerve; a field block can be performed in this region, resulting in complete anesthesia of the external pinna (Figure 2).
The innervations of the meatus and external canal are supplied by the vagus nerve and are very difficult to anesthetize without infiltrating directly into the tissues of the canal. This is usually not necessary for common repairs of the pinna. Epinephrine should not be used with local anesthesia of the ear.
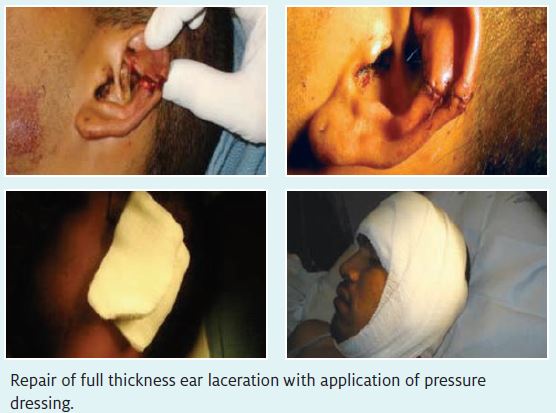
After anesthesia is obtained, irrigation is performed; take care not to damage tissue. Exploration will reveal foreign bodies and the extent of the injury. The layers of the ear must be carefully approximated to assure complete coverage of the cartilage and restoration of normal anatomic relationships so that vascular supply is re-established.
Repair should utilize interrupted fine nonabsorbable sutures. It may be necessary to anatomically align larger wounds with a suture through the cartilage since the perichondrium suture is so thin. In general, if the laceration is extensive and involves the cartilage it is only prudent to consider referral or consultation with a plastic surgeon. Exposed cartilage needs to be fully covered to avoid infection. Tissue and cartilage debridement should be avoided as much as possible (Figure 3).
Dressing the ear can be a bit complex. Patients will not tolerate a dressing that hyperflexes or extends the pinna. Therefore, it is necessary to protect the ear by building a layer of cotton puffs posterior to the pinna to maintain its normal position. A layer of gauze or wrap can be applied exterior to these. Many lacerations can be left open with no dressing other than a layer of antibiotic ointment or petroleum jelly. These lacerations do not require prophylactic antibiotics.
Nose
Cosmetically, the nose acts as the central point of symmetry in the face, and disfigurement can have significant cosmetic consequences. Evaluation of blunt injury to the nose includes a search for injuries to the bony and cartilaginous structures, e.g., the septum, as well as the sinuses and the facial bones.
Most nasal fractures stop bleeding. A stubbornly persistent ooze may represent cerebrospinal fluid rhinorrhea from a cribriform plate fracture. This, like otorrhea, can be tested for with a piece of filter paper or tissue, looking for a layering out of the ooze. This would indicate a head CT scan, and a neurosurgical consultation. These patients do not require prophylactic antibiotics.
Anesthesia of the nose sometimes requires anesthesia of the septum, as well as the soft tissue around the laceration and the epithelium of the laceration. Regional blocks, while useful, are hard to achieve because of the diversity of the innervation of the area. You may not be able to manage complex injuries with local anesthesia. Such patients should have procedural sedation or general anesthesia and may need to be referred to the ED or operating room. These lacerations may require plastic surgery consultation. Topical anesthesia of the nasal mucosa is often adequate for nasal packing. Local anesthetic infiltration of the nose should not include epinephrine.
Nasal lacerations either involve superficial skin only or are complex, including cartilage and bony elements of the nose. Superficial lacerations can be closed with fine non-absorbable sutures.
The physician should look for a septal hematoma, septal deviation, or nasal fracture. If present, these will need to be treated because they represent an open fracture. Many ENTs and plastic surgeons prefer to reduce septal deviations acutely. A septal hematoma needs to be drained to prevent necrosis of the septum. Needle aspiration is rarely successful since the hematoma often recurs. An incision should be made in the mucosa and the anterior chamber packed over a petroleum jelly gauze dressing.
Bilateral septal hematomas should be referred to the ENT or plastic surgeon, and not managed in the urgent care center. Through and through, lacerations of the nose are rarely isolated injuries, and are best referred and repaired by an ENT or plastic surgeon.
Summary
Common head lacerations can be managed by physicians in urgent care setting if careful attention is given to anatomical considerations. Cosmesis is a significant patient concern.
References
- Singer AJ, Thode JC Jr., Hollander JE. National trends in ED lacerations between 1992 and 2002. Am J Emerg Med. 2006; 24(2): 183-188.
- Gaufberg SV, Walta MJ, Workman TP. Expanding the use of topical anesthesia in wound management: Sequential layered application of topical lidocaine with epinephrine. Am J Emerg Med. May 2007; 25(4): 379-384.
- Fariss BL, Foresman PA, Rodeheaver GT, et al. Anesthetic properties and toxicity of bupivaccine and lidocaine for infiltration anesthesia. J Emerg Med. 1987; 5(4): 275-282.
- Moscati RM, Mayrose J, Reardon RF, et al. A multicenter comparison of tap water versus sterile saline for wound irrigation. Acad Emerg Med. 2007; 14(5): 404-409.
- Bender JS. Factors influencing outcome in delayed primary closure of contaminated abdominal wounds: A prospective analysis of 181 consecutive patients. Am Surg. 2003; 69(3): 252-255; discussion 255-256.
- Brown DJ, Jaffe JE, Henson JK. Advanced laceration management. Emerg Med Clin North Am, 2007; 25(1): 83-99.
- Farion KJ, Osmond MH, Hartling L, et al. Tissue adhesives for traumatic lacerations: A systematic review of randomized controlled trials. Acad Emerg Med. 2003; 10(2):110-118.
- Handschel JG, Depprich RA, Dirksen D, et al. A prospective comparison of octyl-2-cyano-acrylate and suture in standardized facial wounds. Int J Oral Maxillofac Surg. 2006; 35(4): 318-323.
- Karounis H, Gouin S, Eisman H, et al. A randomized, controlled trial comparing long-term cosmetic outcomes of traumatic pediatric lacerations repaired with absorbable plain gut versus nonabsorbable nylon sutures. Acad Emerg Med. 2004; 11(7): 730-735.
- Talan DA, Abrahamian FM, Moran GJ, et al. Tetanus immunity and physician compliance with tetanus prophylaxis practices among emergency department patients presenting with wounds. Ann Emerg Med. Mar 2004; 43(3): 305-314.
- Tetanus – Puerto Rico, 2002. MMWR Morb Mortal Wkly Rep. 2002; 51(28): 613-615.
- Epidemiology & Prevention of Vaccine Preventable Diseases. 8th ed; 2004.
- Pascual FB, McGinley EL, Zanardi LR, et al. Tetanus surveillance – United States, 1998-2000. MMWR Surveill Summ. 2003; 52 (3): 1-8.
- Salem GA. Regional anesthesia for office procedures: part I. Head and neck surgeries. Am Fam Physician. 2004; 69(3): 585-590.