Published on
Urgent message: Urgent care clinicians should consider the possibility of cholecystitis when evaluating patients with cardiac symptoms. A delay in diagnosis may lead to serious complications, including sepsis.
ALONA D. ANGOSTA, PhD, APRN, NP-C, and BRYAN HOLMES, NREMTP
Introduction
Patients with acute cholecystitis typically complain of right-upper-quadrant pain that radiates to the right shoulder and back, fever, and leukocytosis.1 The pain may also be associated with nausea or vomiting. However, acute cholecystitis can mimic cardiac symptoms such as chest pain, nausea, and electrocardiogram (ECG) changes.1-5 Conversely, there are other conditions associated with ECG abnormalities that can mimic cardiac pathologies, including acute pancreatitis,6-10 peptic ulcer disease,11, 12 and pneumonitis.4 With the atypical presentations of acute cholecystitis and ECG changes, it can make diagnosis challenging.
Although the association and exact pathophysiologic mechanisms of ECG changes in non-cardiac conditions are poorly understood, multiple hypotheses have been reported, including vagal reflexes, disturbance of coronary blood flow, and coronary vasospasm.11 The aims of this report are to discuss an unusual presentation of acute cholecystitis, provide a discussion of similar cases from evidence-based literature, and offer clinical pearls for the urgent care clinician.
Case Presentation
A 36-year-old white female presented with sudden-onset substernal chest pain associated with palpitations and nausea. The patient was awakened by pain in her chest, which she described as heaviness and pressure without radiation. There was no dyspnea or pain during inspiration, no hematemesis or melena. A pain score of 10/10 was provided by the patient without exacerbating or relieving factors. Her past medical history was unremarkable except for asthma and eczema. Family history was positive for coronary artery disease, diabetes, and hypertension. Social history was negative for nicotine, alcohol, or drug use. Her medications included an albuterol inhaler.
Observation and Findings
During evaluation, the patient had the following vital signs:
- BP: 133/76
- P: 54
- R: 22
- T: 98.1ºF
- O2 sat: 99%
- Wt: 174 lb
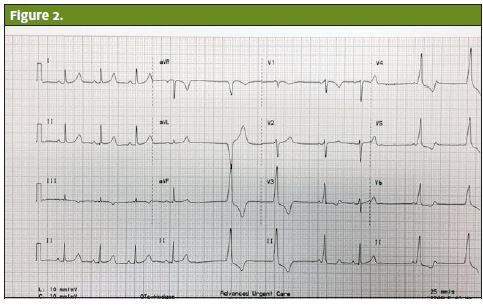
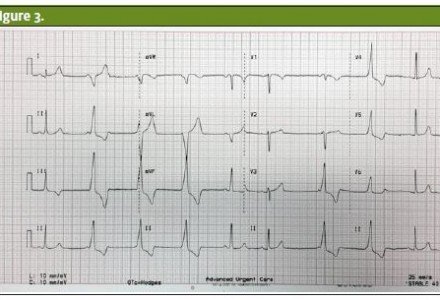
On examination, the patient was anxious and her skin was clammy and cool to the touch. Her lungs were clear to auscultation bilaterally. Her heart rate was bradycardic and the rhythm was irregular. She did not have cardiac murmurs or heaves; no jugular venous distention was noted. The woman’s abdomen was soft, with good bowel sounds without tenderness or masses. A 12-lead ECG revealed sinus bradycardia with frequent premature ventricular contractions (PVCs) (Figures 1-3).
Disposition
Due to the severity and nature of the patient’s pain, and ECG abnormalities, she was transferred immediately to the nearest emergency department (ED) by emergency medical services. Upon ED presentation, the patient complained of increasing epigastric pain and decreasing chest pain, although she continued to show ECG abnormalities with bigeminal PVCs. Laboratory studies including troponins were normal (<0.01) except for a slightly elevated WBC count of 14.4. An abdominal ultrasound was ordered and showed cholelithiasis with gallbladder wall thickening, gallstones, sludge, and pericholecystic fluid. According to Steel and Brenner (2013), ultrasonography has about 90% to 95% sensitivity and 78% to 80% specificity for cholecystitis. For cholelithiasis, it is 98% sensitive and specific.13 Given the elevated WBC and abnormal ultrasound, the patient underwent a laparoscopic cholecystectomy. The pathology report confirmed cholecystitis. The patient was completely asymptomatic post-surgery. Furthermore, ECG changes did not recur. Contact was made with the patient several weeks after hospital discharge. She reported a full, successful recovery, and continued to remain asymptomatic without any further cardiac-related complaints.
Discussion
ECG changes (both non-ischemic and ischemic) in acute cholecystitis have been reported in the literature.14 Franzel et al. reported a case of acute cholecystitis with ECG abnormalities and syncope.15 The case was a 48-year-old male who had severe abdominal pain and syncopal episode. He was bradycardic and his ECG showed complete atrioventricular (AV) block. He was treated for cholecystitis.
Postoperatively, his ECG showed normal sinus rhythm without AV block or arrhythmias. His cardiac workup including echocardiogram was unremarkable. He did not have complications and he was discharged home in stable condition. Another case was reported by Akyel et al. of a 35-year-old male who complained of upper abdominal pain, nausea, and vomiting. His heart rate was 54 beats per minute and his ECG showed idioventricular rhythm. The patient was treated appropriately for cholecystitis and his symptoms resolved.
Bradycardia in acute cholecystitis, also known as the Cope’s sign,16 has been observed in several cases including this case report. In addition, ECG changes have been reported. Although the exact etiology of bradycardia and ECG changes in cholecystitis is not well understood, the suspected etiology is excessive vagal stimulation.17 O’Reilly and Krauthamer indicate that “abdominal pain and gallbladder distention may aggravate vagal discharge and accordingly, bradycardia or conduction disturbances develop.”16
Ischemic ECG changes have also been observed in acute cholecystitis. Aksay et al. reported a 42-year-old male with acute cholecystitis. The patient had epigastric pain, nausea, and vomiting and had T wave inversion on his ECG.2 Following treatment, his symptoms and ECG changes resolved. The investigators believed that the ECG abnormalities were most likely due to the changes in myocardial blood flow rather than persistent coronary artery stenosis or atherosclerosis.2
A similar case was reported by Patel et al. of a 34-yearold white female who had acute cholecystitis.4 The patient complained of epigastric pain, bilateral posterior thorax pain, nausea, and vomiting, and was found to have ST segment elevations on her ECG. Following laparoscopic cholecystectomy, the patient had a full resolution of the ST changes.4 Patel et al. indicated that the inflammation and distention of the gallbladder caused the ECG abnormalities.4 They concluded that irritation and spasticity of the surrounding structures creates reflex stimuli through the autonomic pathways, which leads to temporary alteration in coronary blood supply and causes conduction disturbances.4 Demarchi et al. also reported a case involving a 75-year-old female who presented with acute cholecystitis.1 The patient had ST segment depression on her ECG and elevated troponin levels. Following treatment, the patient’s symptoms disappeared.
1 Demarchi et al. suspected that the ECG changes and abnormal troponin levels were due to the inflammation and distention of the gallbladder.1 In addition, gallbladder pain stimulates the vagus nerve, which in turn causes bradycardia. The pathophysiologic changes in gallbladder inflammation may reduce coronary blood flow and accordingly, troponin levels and
abnormalities in the conduction system may occur.1
References
- Demarchi MS, Regusci L, Fasolini F. Electrocardiographic changes and false-positive troponin I in a patient with acute cholecystitis. Case Rep Gastroenterol. 2012;6:410-414. doi:10.1159/000339965
- Aksay E, Ersel M, Kiyan S, Musalar E, Gungor H. Acute coronary syndrome mimicked by acute cholecystitis. EMA. 2010; 22: 343-346. doi: 10.1111/j.1742-6723.2010.01291.x
- Krasna MJ, Flancbaum L. Electrocardiographic changes in cardiac patients with acute gallbladder disease. Am Surg. 1986;52:541-543.
- Patel N, Ariyarathenam A, Davies W, Harris A. Acute cholecystitis leading to ischemic ECG changes in a patient with no underlying cardiac disease. JSLS. 2011;15:105-108.
- Ryan ET, Pak PH, DeSanctis RW. Myocardial infarction mimicked by acute cholecystitis. Ann Intern Med. 1992;116:218–220.
- Albrecht CA, Laws FA. ST segment elevation pattern of acute myocardial infarction induced by acute pancreatitis. Cardiol Rev. 2003;11(3):147-151.
- Khairy P, Marsolais P. Pancreatitis with electrocardiographic changes mimicking acute myocardial infarction. Can J Gastroenterol. 2001;15(8):522-526.
- Makaryus AN, Adedeji O, Ali SK. Acute pancreatitis presenting as acute inferior wall ST-segment elevations on electrocardiography. Am J Emerg Med. 2008;26:734.e1-734.e4.
- Wu CH, Wang KL, Lu TM. Perplexing epigastric pain-coincident myocardial infarction and acute pancreatitis. Intern Med. 2010;49:149-153.
- Yegneswaran B, Kostis Jb, Pitchumoni CS. Cardiovascular manifestations of acute pancreatitis. J Crit Care. 2011; 26: 225e11-225e18. doi:10.1016/j.jcrc.2010.10.013
- Oguzturk H, Turtay MG, Tekin YK, Tekin G. The evaluation of electrocardiogram findings in acute abdominal pain patients admitted to the emergency department. J Prim Care. 2011;2(3):163-166. doi: 10.1177/2150131911403931
- Sole D, McCabe JL, Wolfson AB. ECG changes with perforated duodenal ulcer mimicking acute cardiac ischemia. Am J Emerg Med. 1996;14(4):410-413.
- Steel AD, Brenner, BE. Acute cholecystitis and biliary colic. Emedicine. Web. 29 Oct. 2014. http://emedicine.medscape.com/article/1950020-overview#aw2aab6b8
- Khair RZ, Ibrahim MT, Malik NM. Improvement of ECG changes in patients with cholelithiasis after cholecystectomy. IJEST. 2014;3(3):1076-1082.
- Franzen D, Jung S, Fatio R, Brunckhorst CB. Complete atrioventricular block in a patient with acute cholecystitis: a case of cardio-biliary reflex? Eur J Emerg Med. 2009;16:346-347.
- O’Reilly MV, Krauthamer MJ. ‘‘Cope’s sign’’ and reflex bradycardia in two patients with cholecystitis. Br Med J. 1971;2(5754):146.
- Akyel A, Yayla C Kunak T, Yaman B, Tavil Y, Boyaci B. Idioventricular rhythm in a patient with acute cholecystitis. Clin Res Hepatol Gastroenterol. 2011; 35(11):774-776. doi:10.1016/j.clinre.2011.07.014