Published on
Urgent message: Rashes are a common ailment, and their etiology can have overlapping appearances. In a case where rash does not improve with treatment, it is often necessary to reconsider the differential.
Sergio Ramoa MD, MS
INTRODUCTION
It is common for providers to have difficulty diagnosing patients who present with rash due to the diverse appearances, as well as overlapping similarities, of different etiologies. Due to the extensive nature of rashes, this article will focus on pediatric rashes that tend to develop in late winter and early spring, as well as the approach to the diagnosis of rashes and tools that can be used. With the volume of pediatric skin concerns being over 12 million visits a year and overlapping characteristics of rash, efficient history taking is essential.1
CASE PRESENTATION
The patient is a 3-year-old male with no past medical history, presenting with his mother with a red rash on the back of his neck. The boy had developed another rash 2 weeks prior. His pediatrician saw him at that time, and was concerned for sun toxicity. The family placed the boy in long-sleeved clothing and hats with sun guards for the neck during outdoor activities. With time, the original rash dissipated. The current rash started the day before this visit and involved the same location of the neck but with bilateral axilla rashes. Mother states that the rash appeared slightly itchy and that he had a mild increase in irritability. She is uncertain when the irritability started with regard to timing of the rash. Family had new detergent at home but denied washing his clothes in them. She denied sore throat, change in appetite, or new animal exposures. He had no recent introduction to new food. When going outside with his protective clothing, she denied him being around or playing with plants. No other family members in the home have a rash or have history of rash.
Physical Exam
- Temperature 98.6⁰, pulse 115, respiration 22/min, O2 saturation 97%, weight 13.42 kg, height 28 inches, BMI 26.6
- Erythematous papules along the posterior neck and bilateral axilla. Scalp spared from rash. Rest of the body spared from rash
- Increased erythema along the axillary fold lines
- Pharynx and tongue without increased erythema. Tonsils with mild injection, no swelling, and no exudates
- Cervical lymph nodes are focal and nontender
- Fair-skinned
- No fluorescent changes under Wood’s lamp
DIFFERENTIAL AND DECISION-MAKING
- The patient is fair-skinned, with light eyes, placing him in a Fitzpatrick skin phototype II. Owing to his skin phototype, he does have a propensity for sunburns; his family took interventions to reduce that, such as long clothing and a hat with neck guard. His new rash in the axilla with torso spared would also decrease concern for sunburn. Sun allergy or sun poisoning could have been a source from the original rash. Correspondingly, the safeguards the family placed should reduce the risk, as it often occurs on sun exposed areas. The rash with sun allergy is polymorphic, while his current rash shows papules.
- Chemical dermatitis is also less likely due to location and rash shape. Irritants such as found in poison ivy, poison oak, or giant hogweed would appear more linear or sometimes even brush stroked on the skin and more likely on the limbs than the torso and neck.
- In children, another inflammatory rash, atopic dermatitis, could present as scaling, vesicles, dry skin, erythematous plaques, and papules. Roughly 20% of children in the United States are affected.1 Typical presentation is aberrant in early childhood and distribution on the body changes depending on the patient’s age. Adults present with rash on flexor surfaces but in children it can be demonstrated on the cheeks, scalp, and extensor surfaces. In our patient, his rash demonstrated more on the flexure points, axilla and nape of neck, and did have erythematous papules present. He and his family have no previous history of rash typical of eczema. He was spared from the rash in the harsh dry winter air, and depending on the potential eczema type, the increase in sun exposure would improve atopic dermatitis. The spring season could introduce allergens that would trigger an atopic dermatitis reaction, especially with his increased outdoor activity.
- For fungal associated rashes, the locations of his rash are typical of seborrheic dermatitis as there are higher density sebaceous glands near the axilla. The irritation from the inflammatory response to the yeast on the skin could also contribute to the erythema and itching. His rash lacked the typical flaking scales. Similarly, tinea corporis could also produce rash and itching and is one of the most common rash in children in the U.S.1 The homogenous appearance of the rash, lacking the erythematous annular with central clearing, symmetry on the body, and lack of scaling with associated hair loss, decreases this likelihood.
- Bacterial sources to the rash could include impetigo and strep scarlet fever. Impetigo can present as bullous or nonbullous type. By skin-to-skin exposure, it can be seeded on the body causing further lesions with a predisposition on the face and extremities. The patient’s rash lacked any yellow crusting and there was no sick contact history that would predispose him.
- Streptococcal scarlet fever typically presents with sore throat and fever 1 to 2 days prior to rash developing. In children, this can sometimes present with gastrointestinal symptoms and lack the textbook pharyngitis. Its rash is a coalescent, erythematous papule resembling a sunburn with sandpaper feel. His rash was previously confused with sunburn, but he lacked the characteristic sore throat or fever.
DIAGNOSIS
Scarlet Fever
Streptococcus type A antigens, by an immunoassay with direct optical observation positive. Throat cultures have a sensitivity of 90% to 95% and, depending on the rapid antigen test, sensitivity ranges from 70% to 90%.1
In the case of this patient, he was 3 years old and did have an atypical presentation of streptococcal pharyngitis. Prior to a rash developing he only had increased fussiness. This would have allowed the infection to persist unknown, except that it manifested into scarlet fever. It first showed at flexure surfaces and the head, which is typical of scarlet fever before it distributes further across the body. The rash appears 12 to 48 hours after infection. If rash is along creased body surface, it has increased erythema called Pastia lines. The patient had Pastia lines in bilateral axilla.
After the diagnosis, the mother recalled that her husband was recently seen and treated for strep throat. Group A beta-hemolytic streptococcal (GABHS) is a common cause of pharyngitis in children, comprising approximately 30% of cases in ages 5 to 15 and about 5%-10% in adults.2 Streptococcal pharyngitis can be uncommon in children younger than 3 and may present with prolonged symptoms such as irritability, rhinitis, anorexia, and fevers. GABHS is spread by respiratory droplets and sometimes direct physical inoculation. Symptoms can present 2 to 5 days after inoculation.3 The toxin mediated exanthem is caused by a pyrogenic exotoxin producing S pyogenes. Incidence of scarlet fever in those with streptococcal-induced tonsillopharyngitis in the United States is not known, as this is not surveyed by the CDC. Globally, there have been recent outbreaks in China, Australia, and the United Kingdom.
TREATMENT
The penicillin class still has high effectiveness against streptococcal species, as do beta-lactam antimicrobial agents. Oral treatment of choice is penicillin V, 400,000 U if less than 27 kg and 800,000 U for about two to three times a day for 10 days, or amoxicillin 50 mg/kg once or divided into twice daily for a maximum of 1000 mg for 10 days. For those unable to tolerate PO, penicillin G benzathine, 600,000 U for children less than 27 kg and 1.2 million U for those above 27 kg, can be given as a one-time injection. For those with penicillin allergies, clindamycin or a first-generation cephalosporin (such as cephalexin) can be used for the next line of treatment. Macrolides are another alternative to those that have penicillin allergy, but resistance rates are as high as 5% to 10% in most areas of the U.S.3 Sulfonamides and tetracyclines should not be used as treatment for GABHS.2
If reoccurrence of symptoms and infection occur shortly after treatment, the same, original medication or a different medication can be used. If symptoms continue to recur, at that time it will be important to differentiate from repeat GABHS infection or carrier with recurring viral pharyngitis.
Carriers of GABHS are less likely to transmit infection to others, are not at risk for complications, and do not need to be treated.3,4 Though carriers are not routinely treated, specific circumstances call on eradication. These include: community outbreaks, family history of rheumatic fever or rheumatic heart disease, local outbreak of acute rheumatic fever or poststreptococcal glomerulonephritis, and back-and-forth passage of infection within a family despite adequate treatment.3,4 Carrier status can be difficult to resolve, and supplemental treatment is needed along with the standard 10-day penicillin treatment. Amoxicillin-clavulanate, the antibiotic treatment options mentioned above, or a penicillin with rifampin for the last 4 days of treatment were more effective than penicillin alone for treatment of a chronic carrier state.3,4
DISCUSSION
Skin phototype can vastly change the appearance of a rash. This patient was fair-skinned and an erythematous rash was well appreciated. In a higher Fitzpatrick skin phototype, redness may not be as well appreciated. Even with the differential of tinea and seborrheic dermatitis, a phototype VI could have an opposite appearance. Red or darker patches may show on light skin and lighter patches on dark skin. With evaluation of rashes, it is important to take quick note of distribution of lesions, arrangement, color, and primary vs secondary changes to make an accurate diagnosis. In the cases of indistinguishable rashes, history of exposures to plants or insects; drugs that are prescription, herbal, or supplemental; pets; hobbies; chronic history; travel; immunization history; and other sick contacts should be fully detailed.
Your own senses are the most powerful tools to gather details from a rash, but a Wood’s lamp and dermoscope can assist in diagnosis.
The dermoscope can detect subsurface characteristics through a transilluminating light source. With appropriate training, physicians were able to more accurately identify cancerous skin lesions and improve referral rates for excision.5 The skin contains numerous compounds such as collagen, elastin, and coenzymes that can become fluorescent under UV light.6
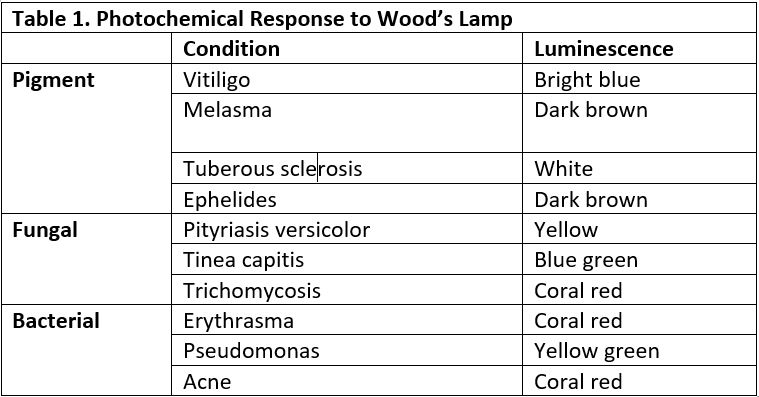
When using a Wood’s lamp, some of the greatest benefits come from examination of pigment disorders and infections of the skin. For instance, melanin absorbs UV light directed at the skin. In cases of vitiligo and melasma where there is hypopigmentation and hyperpigmentation, respectively, a Wood’s lamp can clearly demarcate the circumference of the lesion, even when subtle.

As noted in Table 1, a photochemical response can better distinguish between hypopigmented lesions, as vitiligo has a blue-white appearance, pityriasis versicolor demonstrates yellow gold, and tuberous sclerosis appears white.6 Cutibacterium acnes, formerly propionibacterium acnes, can be found in the bacterial skin flora. In a case where there is a mild acne presentation that needs to be distinguished from milia, the Wood’s lamp can guide to an appropriate diagnosis. The fluorescence cutibacterium acnes produces is coral red, and can be found concentrated in follicles and comedones, particularly on the face. The Wood’s lamp is a simple device that can give immediate character details for a rash.
Scarlet fever is also known as scarlatina and second disease. It has been recorded as far back as the 1500s. Previous historical records demonstrate scarlet fever as a devastating disease with mortality rate as high as 30%.7 Due to improved access to medical care, appropriate antibiotic treatment, and improved nutrition, the occurrence of GABHS related disease has dramatically declined.7,8 Despite the change in mortality rate, however, GABHS causes 500,000 deaths and 700 million illnesses a year worldwide.8 Scarlet fever requires susceptibility of the host to the pyrogenic exotoxin. Children younger than 2 years old may have maternal antibody protection, and 80% of children by 10 years old have lifelong antibodies against the exotoxins.4
Scarlet fever rash is a fine, popular, erythematous rash typically on the trunk that spares the palms and soles while spreading throughout the body starting at the head. The rash is often described as “sandpaper” or a sunburn. It lasts up to 10 days and after resolution can have desquamation that lasts up to 6 weeks.2 Pastia lines occur where there is increased erythema along skin folds. The rash is often accompanied by fevers, sore throat, and swollen tongue papillae with white coating or redness if the white has desquamated. Antibiotic treatment can expedite resolution of symptoms and decrease the contagious window from 1-2 weeks after symptoms began to 24 hours.
There are several mimickers to scarlet fever. If fevers persist for 5 days despite treatment, it’s important to consider Kawasaki’s disease, which has additional exam findings such as conjunctivitis; red, dry cracked lips and tongue; and red, swollen hands and feet that can later desquamate. Streptococcal scarlet fever can be differentiated from staphylococcal scarlet fever by the lack or strawberry tongue (Figure 2) and circumoral pallor. The skin rash in staphylococcal-induced scarlet fever is painful. Rash that spreads cephalocaudally can also be concerning for rubella and rubeola. Both tend to have coryza, conjunctivitis, and cough. In comparison to scarlet fever, measles symptoms begin 7 to 14 days after infection. Tiny white spots in the mouth, Koplik spots, appear 3 days after symptoms begin. The erythematous papules of the skin may join together as they spread through the body. With rubella, rash is typically the first symptom; other symptoms such as low-grade fever, sore throat, and mild pink eye are mild in children.

TAKE-HOME POINTS
- Rapid antigen testing sensitivity ranges from 70%to 90%; specificity is 95%
- Severity of scarlet fever has decreased
- Incidence of acute rheumatic fever has declined
- Penicillins, cephalosporins, clindamycin, and macrolides can be used for treatment
- Sulfamethoxazole-trimethoprim and tetracyclines should not be used
- If persistent symptoms, consider Kawasaki disease, staphylococcal scarlet fever, drug rash, rubella, and rubeola
REFERENCES
- Allmon A, Deane K, Martin KL. Common skin rashes in children. Am Fam Physician. 2015;92(3):211-216.
- Cash JC, Glass CA, Mullen J. Family Practice Guidelines. New York, NY, New York: Springer Publishing Company; 2021.
- Kimberlin DW, ed. Red Book: 2018-2021 Report of the Committee on Infectious Diseases. 31st ed. American Academy of Pediatrics. 2018.
- Martin J. The Streptococcus pyogenes carrier state. In: Ferretti JJ, Stevens DL, Fischetti VA, ed. Streptococcus pyogenes : Basic Biology to Clinical Manifestations. Oklahoma City, OK: University of Oklahoma Health Sciences Center; 2016.
- Marghoob AA, Usatine RP, Jaimes N. Dermoscopy for the family physician. Am Fam Physician. 2013;88(7):441-450.
- Klatte JL, van der Beek N, Kemperman PM. 100 years of Wood’s lamp revised. J Eur Acad Dermatol Venereol. 2015;29(5):842-847.
- Lee GM, Wessels MR. Changing epidemiology of acute rheumatic fever in the United States. Clin Infect Dis. 2006;42(4):448-450.
- Maness DL, Martin M, Mitchell G. Poststreptococcal illness: recognition and management. Am Fam Physician. 2018;97(8):517-522.
Author affiliation: Sergio P. Ramoa MD, MS, CareNow Urgent Care HealthONE Denver, CO.