Published on
Urgent message: Assessment of patients presenting with psychiatric conditions requires amodified set of skills compared with traditional medical assessment. Urgent care clinicians must be prepared to determine appropriate interventions—treatment, referral, or both.
Gregory P. Brown, MD
Introduction
Typically, the interaction between clinicians and patients presenting with psychiatric conditions is guided by information obtained from the interview, history, and physical examination rather than emphasizing laboratory or radiological testing. Therapeutic options may be challenged by a lack of community resources in many regions of the country.
The general model, however, for the evaluation of a psychiatric patient in urgent care settings remains similar in overall format to that of a traditional medical patient:
- assessment of the condition
- appropriate intervention for the presenting com- plaint
- disposition to an alternative level of care when appropriate.
The importance of skill in assessment, intervention, and disposition of the patient with psychiatric complaints cannot be over- stated, as it is estimated that at least 40% of patients presenting in an urgent care or primacy care setting have some symptoms which can be appropriately categorized as “mental health-related.”
While not exhaustive, this article will provide reasonable, general concepts for this type of evaluation.
Assessment
The assessment of a psychiatric patient requires a thorough description of current and past symptoms of the nature that brought the patient to the urgent care setting, as well as an assessment of the patient’s acuity.
The history-taking is followed by a general mental status and physical examination, with a focus on acute medical conditions and the possible effects of substance use.
| Table 1. Symptoms |
| • Psychosis—reality based? • Anxiety—autonomic hyper-arousal? • Mood—dysphoria or elation? • Cognitive—delirium or dementia? |
Isolating a condition that has been medically induced, such as a mood disorder secondary to hypothyroidism, or one that stems from substances of abuse, such as a cocaine intoxication-induced psychosis, may dramatically alter the intervention and disposition of a patient whose presentation initially suggested a primary psychiatric illness.
The urgent care clinician does not need to memorize the entirety of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV), but rather can focus inquiry on the degree of symptomatology and its acuity. A specific DSM-IV diagnosis may in many cases be beyond the scope of the average urgent care clinician with little or no formal psychiatric training.
The main categories of symptoms likely to present within the urgent care setting include psychosis, anxiety, mood alterations, or cognitive impairment. Each carries with it a set of symptoms (Table 1), physical findings, and secondary evaluations that will help inform intervention. Psychosis symptoms are characterized by hallucinations or delusions—both substantial departures from consensual reality. Depending on the content of the psychotic features, agitation or paranoia may also be prominent; this could require more urgent intervention. Psychosis can also present as marked confusion with disorganized thinking leading to substantial inability to provide even basic self-care.
Anxiety symptoms may be related to hyper-responsiveness of the sympathetic nervous system. The most intense version of anxiety symptoms is a panic attack, which often includes a sense of doom, shortness of breath, chest tightness, diaphoresis, and palpitations. These symptoms may be confused by both the patient and the physician with a myocardial infarction or pulmonary embolism. In turn, an MI or PE often presents with acute anxiety. The differentiation can be challenging and may require a level of care beyond that available in the urgent care setting.
Panic attacks may be a symptom of several different anxiety disorders. In the urgent care setting, the primary goal is to alleviate symptoms of the actual panic attack and assure appropriate follow-up.
Mood symptoms are likely to be those of depression or of mania, opposite ends of the spectrum. Specific focus on assessment of any suicidal thoughts and plans are especially important when mood symptoms are the primary presenting issue.
Currently, the diagnostic criteria of bipolar disorder have come to be too often loosely applied; some caution should be used in accepting this history in the absence of a careful psychiatric review of systems.
Cognitive impairments in the urgent care setting typically involve changes in mental status consistent with either acute delirium or acute deterioration of a chronic dementing condition. Should the patient present with new cognitive symptoms or a clouding of consciousness suggestive of either dementia or delirium, respectively, these conditions must be properly evaluated and stabilized medically prior to transfer to a psychiatric facility. Acute delirium should be considered a medical emergency even if confusion or apparent psychiatric symptoms are present. The medical cause of acute delirium must be sought and stabilized prior to a complete psychiatric evaluation.
Briefly, delirium is an acute confusional state characterized by a decreased ability to focus, sustain, or shift attention. Symptoms usually wax and wane. Dementia, on the other hand, is more of a steadily progressive disorder without rapid fluctuations in the absence of a new stressor such as medications or infections.
It is essential to obtain the medical–psychiatric history of an individual presenting with apparent psychiatric diagnoses or complaints. Obtaining the previous psychiatric diagnosis can be useful, especially a review of the interventions which were successful in the past.
It is also important to assess whether the presenting condition is chronic or acute. A chronic condition may be managed quite effectively at a lower level of care, especially with supportive family members or community. Always be vigilant for a new, reversible problem that may be worsening a chronic condition.
Substance-induced mood disorders or substance- induced psychoses require observation for a period of time adequate for the specific substance to clear prior to making a diagnosis of an independent psychiatric condition.
Medications prescribed for both psychiatric and medical conditions can cause psychiatric symptoms, including delirium. Careful consideration of newly added or recently stopped medications is essential when assessing new-onset psychiatric symptoms.
Intervention
The interventions for patients presenting with psychiatric complaints tend to be pharmacological, psychological, social, and/or medical.
For the patient who presents with an acute psychosis— either hallucinations or delusions combined with severe agitation—a combination of medications can be given. Typically, this would include a combination of 5mg of haloperidol (Haldol), 2mg of lorazepam (Ativan), and 50 mg of diphenhydramine HCl (Benadryl), either PO or IM. The expectation is that this combination, known colloquially as “B52,” will cause sedation, not resolve the underlying psychosis.
Note that it is essential to give the haloperidol in combination with the lorazepam and diphenhydramine; this combination acts to prevent acute dystonic reactions that increase agitation and can be confused with worsening of psychosis.
If agitation is the primary difficulty, this combination can be repeated once or twice at 30- to 60- minute intervals until agitation is resolved or until the patient can be appropriately transferred to a higher acuity type facility.
Table 2 offers an overview of options based on the conditions described here.
Panic attack or severe anxiety
For the patient who presents with a panic attack or severe anxiety, a high-potency benzodiazepine such as clonazepam (Klonopin), alprazolam (Xanax) or lorazepam may be used in an acute setting, in concert with a referral for psychiatric services to assess whether or not a more appropriate long term medication and therapy would be preferred.
Depressive disorder
For the patient presenting with symptoms of a depressive disorder, either a selective serotonin reuptake inhibitor (SSRI) or a selective serotonin plus norepinephrine reuptake inhibitormay be the treatment of choice. Whether this is started from the urgent care setting depends on the timing and availability of follow-up with a primary care or psychiatric provider.
Bipolar mania
The patient who presents with a manic syndrome from an established bipolar condition may be treated with divalproex sodium (Depakote) at 50 mg/kg per day and/or a newer atypical antipsychotic medication. Examples of the latter include aripiprazole (Abilify), risperidone (Risperdal), olanzapine (Zyprexa), and others. Contemporaneous consultation with a treating psychiatrist would be ideal in choosing an acute treatment plan, especially when the patient is already on other psychiatric medications.
If this condition is new and not well characterized, or is leading to in- creased agitation, higher levels of care may be necessary.
| Table 2. Pharmacological Interventions | |
| Type of condition | Options |
| Acute psychosis, severe agitation | Haloperidol + lorazepam + diphenhydramine (B52) |
| Panic attack or severe anxiety | Lorazepam, clonazepam, or alprazolam |
| Depression | SSRI or SSNRI |
| Bipolar mania | Divalproex sodium and/or atypical antipsychotic |
| Substance induced | Substance specific |
| Chronic conditions | Condition-specific; restart that which worked best before |
Chronic conditions
When there is a history of chronic psychiatric conditions, the most reason- able intervention may be simply to restart the medication(s) which worked best in the past.
Non-pharmacologic interventions
Non-pharmacologic interventions for the patient presenting with psychiatric complaints include providing a quiet area and time for the individual to decompress and calm down. In addition, building rapport in a non- confrontational manner and providing the patient an opportunity to express feelings and thoughts as fully as possible may allow him/her to re- solve the condition to the point where a higher level of care might be un- necessary.
Social services interventions may as simple as helping the person find a shelter or place to live.
If the individual presents with what may be an acute medical condition that is leading to the psychiatric symptoms, then characterizing and stabilizing the medical condition must be the primary focus of care.
Disposition
The typical disposition choices in most communities include inpatient or outpatient care for medical conditions, psychiatric conditions, or sub- stance detoxification and rehabilitation. Inpatient medical care would be a primary disposition for delirium (e.g., elderly patients who have new-on- set medical problems resulting in changes of mental status; brain injury cases; or post-trauma cases or new-onset medical conditions that have psychiatric symptoms in affiliation).
Inpatient psychiatric care may be appropriate for patients presenting with acute psychosis, suicidal thoughts, or suicidal behaviors and acute manic conditions with psychotic features, especially when self-care is impaired or the diagnosis and effective treatment plan are not well established. In addition, if the person presents in a catatonic state, inpatient psychiatric care may be necessary to provide for ba- sic self-care needs.
Inpatient substance abuse treatment programs would be appropriate if use has been escalating or there is potential for medical instability related to the detoxification process, or unstable vital signs. A substance- induced psychosis that is not rapidly clearing may require inpatient substance treatment.
Outpatient medical treatment of this patient population would include chronic conditions, the management of hormonal imbalances (though perhaps not in the urgent care setting), or follow-up for an acute condition or medication side effect when adequate support is available.
Note that akathisia can present as a side effect of dopamine blocker medications and of phenothiazines often used for gastrointestinal complaints. Its presence is of considerable concern, as it raises suicide risk.
Outpatient psychiatric treatment would be reasonable for many of the patients assessed in terms of continuing or modifying the medications prescribed from the urgent care setting or reassessing the psychiatric condition, and is ideal for non-psychotic, non-acutely dangerous patients. Outpatient psychotherapy may be most appropriate for mood disorders, personality disorders, or those who have an identified acute life stressor.
Outpatient substance abuse programs are now quite common for detoxification and sobriety maintenance for those substances of abuse with non-life threatening withdrawal symptoms, and are ideal for the well-motivated patient.
Challenges
The repeat patient presents a specific challenge in the urgent care setting. Typically, these populations include patients who have been noncompliant with outpatient treatment, have comorbid substance abuse combined with chronic mental illness, and/or comorbid medical illness.
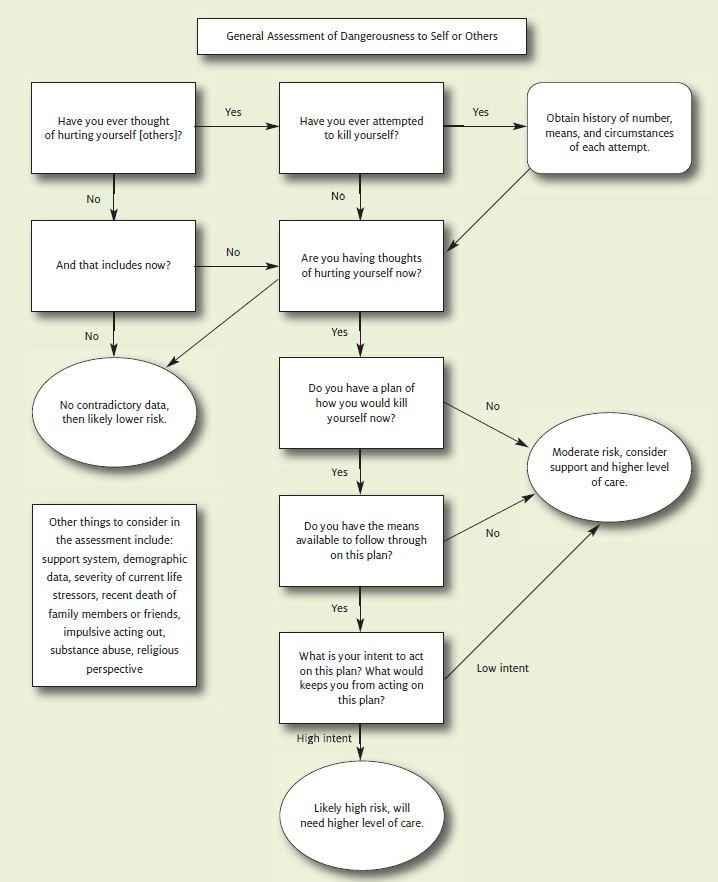
Involuntary commitment statutes are different for each state, but there are some general commonalities. It is important for the urgent care physician to be aware of the legal processes within the state where he/she practices to allow for the involuntary evaluation and retention of a mentally ill individual. Most states require that an individual be both mentally ill and dangerous to either self or others in order to be held for involuntary assessment. A general assessment tool for establishing level of danger to self or others is offered in Figure 1. Some states allow for the combination of mental ill- ness and grave disability for this process.
“Grave disability” is usually defined as such poor ability to care for self that serious bodily harm would result if the patient were not hospitalized. Initially, the decision to hospitalize a patient against his/her expressed wishes is a clinical judgment, but state laws define who can make that initial assessment. After the required judicial review, the final decision becomes a legal finding.
Summary
In summary, the evaluation of the psychiatric patient in the urgent care setting requires that the clinician assess the symptom complex of the patient and rule out or treat acute contributing medical conditions. At times, the resolution of an acute medical condition will also re- solve the psychiatric symptoms, classic examples being hypothyroidism masquerading as a major depressive disorder, encephalitis presenting with delirium, or a cocaine intoxication mimicking the symptoms of schizophrenia or mania.
In the urgent care setting, the physician should pro- vide symptomatic relief of the chief complaint in an appropriate manner, which may include pharmacological, psychological, or social intervention. This is followed by a reasonable disposition plan, as indicated by either the seriousness of the symptom complex or the presence of ongoing acute dangerousness towards self or others.
Share you experience
If you have treated a patient with any of the presentations described in this article, let us know. We will publish relevant case studies in an upcoming issue of JUCM. Send an email to [email protected] for more information
