Published on
Introduction
Appendicitis due to foreign bodies is a rare occurrence; most cases reported in the literature have occurred due to sharp objects such as pins, needles, toothpicks, and small nails.
Solid foreign bodies – such as a bullet – rarely cause appendicitis. Appendicitis due to traumatic gunshot wounds has been described before, as have appendicitis cases due to ingested birdshot.
Here, we describe an interesting case that demonstrates the importance of eliciting a history of ingested food – including wild game – in a patient presenting with symptoms suggestive of appendicitis, particularly in areas of the country where hunting may be an important part of the patient’s lifestyle.
Case Study
A 55-year-old white male presented to our urgent care center with a complaint of progressively worsening right lower quadrant pain, nausea, and a two-day history of anorexia. His most recent meal was squirrel stew, which he prepared for himself, 48 hours before our examination. He reports that he had also shot the squirrel himself two days prior.
The patient denied any diarrhea, constipation, fever, chills, dysuria, or melena. He had taken over-the-counter antacids without relief of his symptoms. His past medical history, surgical history, family history, and social history were otherwise unremarkable and noncontributory.
Findings
On examination, we found this thin male in moderate distress, with:
- BP 140/110 mmHg
- heart rate 120 beats per minute
- T 98.4°F
- respiration 20 per minute.
In addition:
- A CBC revealed a white blood cell count of 11,200, with 82% segs and 2% bands.
- Hemoglobin was 16.4.
- Hematocrit was 38%.
- Platelet count was 450,000.
- Comprehensive metabolic profile (CMP) was normal, except for blood urea nitrogen of 31 mg/dL, creatinine of 1.0 mg/dL, and bicarbonate of 22.
- Urinalysis was unremarkable.
The patient had no jaundice, no oral mucosal lesions, no neck lymphadenopathy, and a normal cardiac examination except for sinus tachycardia. His lungs were clear to auscultation, and he had no thoracic wall tenderness.
The abdomen was not distended, and he had no visible or palpable herniae, and hyperactive bowel sounds in the epigastric area. He was tender to palpation in the periumbilical area and in the right lower quadrant, with point tenderness over McBurney’s area. The psoas sign and obturator sign were negative. He had no involuntary guarding, and no rebound tenderness. Rectal examination revealed no rectal tenderness, no mass, and hemoccult-negative stool. Genitourinary examination was unremarkable.
A flat and upright film of the abdomen revealed no free air, no air-fluid levels, and no signs of obstruction. There was, however, a radiopaque density in the right lower quadrant.
A CT scan of the abdomen and pelvis with thin slices through the appendix revealed a metallic foreign body in the vicinity of the appendix (Figure 1). Bowel gas pattern demonstrated inflammatory changes in the region of the appendix, consistent with acute appendicitis.
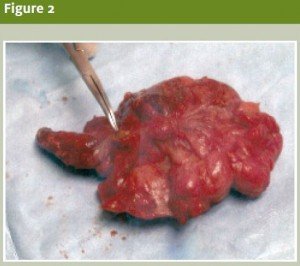
An attending surgeon was consulted, and the patient was emergently transferred, ultimately to be taken to the operating room. Intra-operatively, the surgeon found a .22 caliber rifle slug causing luminal obstruction of the proximal appendix, as well as evidence of early necrosis (Figure 2).
The patient was discharged from the hospital two days later, with an uneventful postoperative course.

Discussion
West Virginia is a true sportsman’s paradise and has numerous seasons for hunting wild game, fishing, and an abundance of outdoor activities.
Typically, squirrels are shot with a small caliber rifle such as a .22 caliber or a 16-or 20-gauge shotgun.
Our patient reported using a .22 caliber rifle to shoot squirrels on the first day of squirrel hunting season. He slaughtered the animals himself, and prepared and cooked the meat, although he did not find d bullet or bullet fragment in the meat. He assumed that the .22 caliber bullet had passed through the animal.
Foreign bodies can cause acute appendicitis by appendiceal lumen obstruction.1,2 Studies have shown that foreign bodies cause appendicitis in 0.0005% of all cases.3 A large number of foreign bodies have been described in the lumen of the appendix; most commonly, these are fruit seed, bone fragments, chewing gum, and gallstones.4 Occasionally, extremely unlikely foreign objects such as fishhooks, dental drill bits, and even a portion of a condom have caused appendiceal lumen obstruction.5
Rare as they may be, most cases of appendicitis caused by a foreign object are found to occur due to sharp foreign objects like the aforementioned pins, needles, toothpicks, and nails.6 Birdshot and similar smooth, round objects have been found in cases of appendicitis, and as many as 500 small shotgun BBs have been reported in the appendix of Inuit Indians who eat wild game as a major part of their diet.7
Most foreign objects pass through the GI tract without any incident, but heavy objects such as a bullet or lead shot from shotguns may have a long transit time – up to two weeks – to transverse the GI tract.8
The position of the appendix is an important risk factor for foreign body obstruction of the lumen, resulting in appendicitis. The anterior position of the appendix rarely is implicated in foreign body-induced appendicitis; however, a retrocecal appendix by virtue of gravity and its dependent position is more likely to become occluded by foreign body resulting in appendicitis.
The ingestion of a foreign body and the development of appendicitis do not go hand in hand. Most of the time, there is a delay (sometimes years) of the onset of symptoms of an ingested foreign body.9
Conclusion
Although most foreign bodies pass through the GI tract without incident, luminal obstruction of the appendix can occur, leading to acute appendicitis. Clinicians are cautioned to be vigilant to this possibility, particularly, in patients presenting with abdominal pain in geographic regions where hunting plays a large part of their lifestyle and diet.
References
- Bach CM, Silver D. Foreign bodies in the appendix. Arch Surg. 1971; 102: 14-20.
- Green SM, Schmidt SP, Rothrock SG. Delayed appendicitis from an ingested foreign body. Am J Emerg Med. 1994; 53-56.
- Sukhotnik I, Klin B, Siplovich L. Foreign body appendicitis. Paediatr Surg. 1995; 30: 1515-1516.
- Collins DC. 71,000 human appendix specimens: A final report, summarizing forty years’ study. Am J Proctol. 1963; 14: 365-381.
- Klingler PJ, Seeling DH, Devault KR. Ingested foreign bodies with the appendix: A 100 year review of the literature. Digest Dis. 1998; 16: 308-314.
- Rubinoff ML. IUD appendicitis. JAMA. 1975; 231(1): 67-68.
- Carey LS. Lead shot appendicitis in northern native people. J Can Assoc Radiol. 1977; 3: 171-174.
- Shade JG, Kronz JD, Rodeberg DA. Foreign bodies within the appendix: A case report and literature review. Contemp Surg. 2000; 36: 10-14.
- Duckler L. Foreign body producing appendicitis. Clin Pediatr. 1976; 15(4): 383.