Published on
David Stern, MD
Q.I read your column about new vs. established patient coding in the January Issue of JUCM. Although the information provided was correct at one time, I believe that Medicare has updated its algorithm to come closer to the algorithm provided by AMA for new vs, established patients.
A.You are correct. In a somewhat obscure and rarely referenced information release. (www.cms.hhs.gov/MLNMattersArticles/downloads/MM4032.pdf) CMS did change its position on this issue. “Physicians should not that this article clarifies and corrects the definition of “new patient” and “physician in a group practice” for billing evaluation and management (E/M) services ….”
The release (which denotes new language in bold and italic) further advises:
“Interpret the phrase “new patient” to mean a patient who has not received any professional services, i.e., evaluation and management (E/M) service or other face-to-face service (e.g., surgical procedure) from the physician or physician group practice (same physician specialty) within the previous three years. For example, if a professional component of a previous procedure is billed in a three-year time period, e.g., a lab interpretation is billed and no E/M service or other face-to-face service with the patient is performed, then this patient remains a new patient for the initial visit. An interpretation of a diagnostic test, reading an x-ray or EKG etc., in the absence of an E/M service or other face-to-face service with the patient does not affect the designation of a new patient.”
Thus, CMS no longer limits the definition of such face-to-face services to those services defined by an E/M code. Now any face-to-face service with a physician will suffice to establish a patient in a practice. This brings the CMS definition of a “new patient” more into line with the AMA (CPT) definition of the “new patient.”
One discrepancy does still exist. CMS restricts the use of the definition of “same physician specialty” to the specific specialties defined by CMS with two-digit physician specialty codes. This list of these specialties and their two-digit designations can be found on the internet at www.cms.hhs.gov/GEM/Downloads/GEMMethodologies.pdf. AMA (CPT), however, does not specifically define what constitutes a physician of “same physician specialty.”
This discrepancy can make a practical difference when a patient is seen in a practice by a physician who is practicing a specialty that is not defined by a two-digit CMS code.
For example, occupational medicine is a recognized specialty with a board certification. CMS, however, does not have a two-digit specification for an “occupational medicine” physician. Board certification is occupational medicine, however, is actually performed by the American Board of Preventative Medicine, and CMS does list specialty code 84 as designating a specialist in occupational medicine.
Thus, if a patient has been evaluated and treated in your urgent care center by a physician who is board certified in occupational medicine (i.e., by the American Board of Preventive Medicine) for an injury covered under workers compensation, and if the patient is subsequently seen for an illness by a physician specializing in family practice, then you may code the second visit with an E/M code for a “new patient.”
If however, the first visit was with a physician specializing in “urgent care medicine.” which CMS does not recognize with a two-digit code, then the second visit would have to be coded as an “established patient” visit.
Under AMA (CPT) rules, we are not limited to a specific, defined list of physician specialties. Again, whether the first visit was with a specialist in occupational medicine or a specialist in urgent care medicine, the second visit might be coded as a “new patient” visit, since the second visit was with a “specialist” in a different specialty.
One might recommend caution, however, when using undefined specialties such as “urgent care” that are not recognized by CMS nor have board certifications that are generally recognized by the medical establishment, as this may place the coded in the uncomfortable position of having to defend the legitimacy of a specialty that is not generally recognized.
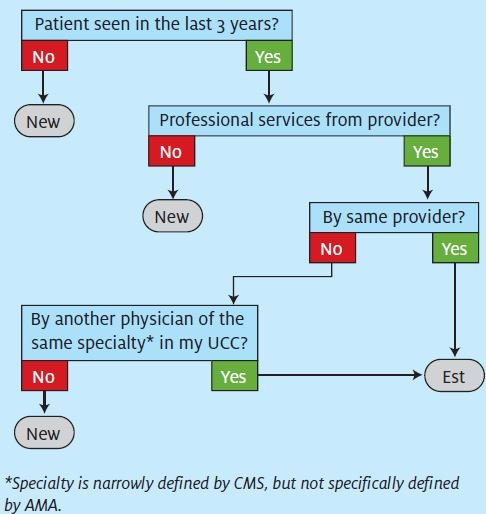
The diagram below updates the one published in the January 2009 issue of JUCM.
Note: CPT codes, descriptions, and other data only are copyright 2007 American Medical Association. All Rights Reserved (or such other date of publication of CPT). CPT is a trademark of the American Medical Association (AMA).
Disclaimer: JUCM and the author provide this information for educational purposes only. The reader should not make any application of this information without consulting with the particular payors in question and/or obtaining appropriate legal advice.
