Published on
Urgent message: Ocular complaints for which there is no immediate, obvious explanation do not necessarily have to be referred to the emergency room or ophthalmology. Employing the process of elimination to narrow down a broad differential, using the available evidence, can expedite the correct diagnosis while allowing the patient to remain in the urgent care.
Kayla Penny, BS; Joseph LaRochelle, PharmD, BCPPS, FCCP; Deirdre Hooper, MD; Haley Caire, BS; and Kelsey Rooney, BS
CASE PRESENTATION
A male in his 40s presented with complaints of an enlarged pupil and blurry vision in his left eye. He reports that his symptoms started about 3 hours ago, following a morning of household chores. Since onset, his symptoms have remained constant and his right eye is not affected. The patient states that he woke up that morning feeling normal and did not notice any pupillary abnormalities.
Of note, he has a history of hyperhidrosis and reports applying a topical medicated wipe to his face just prior to engaging in his household chores. He reports thorough handwashing prior to and following medication application. He denies any atypical exposures while cleaning, including both new cleaning and gardening products. He also denies any trauma during this time. He reports full extraocular movements and denies eye pain, headache, stiff neck, nausea, vomiting, photophobia, seizure, use of blood-thinning medication, numbness, tingling, weakness, and dry mouth. He denies a history of prior similar episodes.
Past Medical History
The patient has a medical history significant for severe hyperhidrosis, GERD, and allergic rhinitis. He denies any surgeries or relevant family history.
Medications
The patient takes fluticasone nasal inhalation (qd), omeprazole (qd), topical cloth glycopyrronium 2.4% applied to the forehead (PRN), botulinum toxin injections to his axilla (quarterly for the last 8 years).
Review of Systems
- Constitutional: denies weight loss/gain, fever, chills, fatigue
- Ear, nose, throat: denies sore throat, rhinitis, tinnitus, and hearing loss
- Gastrointestinal: denies nausea, vomiting, and diarrhea
- Cardiovascular: denies chest pain, palpitations, and edema
- Pulmonary: denies shortness of breath, cough, and wheezing
- Musculoskeletal: denies myalgias, joint pain, and joint stiffness
- Genitourinary: denies hematuria, dysuria, and incontinence
- Psychiatric: denies depression, agitation, and anxiety
- Integumentary: denies rashes, pigmentation, and dryness
Physical Exam
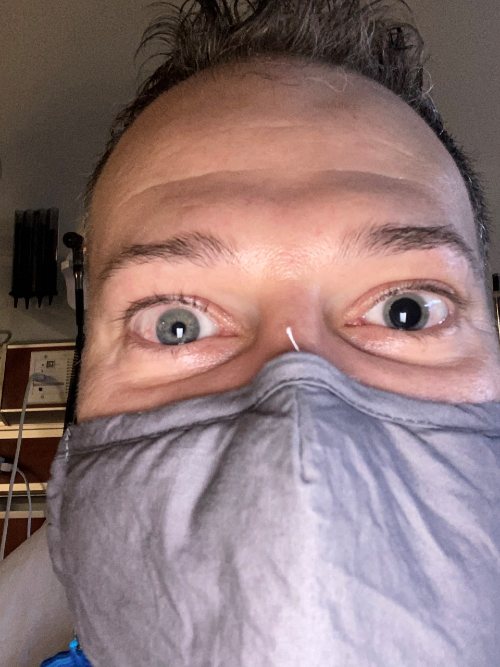
On physical exam, he was hypertensive with a blood pressure of 185/105, but in no apparent distress. The patient was alert, oriented, interactive and well-appearing. The left pupil was enlarged and unreactive to light (Figure 1). Upon further inspection of the left eye, the globe was intact and the conjunctiva were not injected, and no hyphema was noted. Respiratory effort was normal with no apparent wheezing or shortness of breath. Patient had normal range of motion, tone, sensation, and strength in the upper and lower extremities with no rashes, lesions, swelling, or erythema noted.
DIFFERENTIAL DIAGNOSIS
- Medication side effect
- Cerebral aneurysm
- Stroke
- Botulism
- Adie’s syndrome
- Cocaine intoxication
- Recent eye trauma
- Acute-angle closure glaucoma
DIAGNOSIS
Upon detailed review of medications and the patient’s activity on the day of presentation, it is most likely that the mydriatic pupil was a side effect of the glycopyrronium 2.4% cloth he used on his face approximately 2.5 hours prior to noticing blurry vision. Although he followed up application with thorough handwashing, he engaged in strenuous household work, which may have contributed to incidental spread of the medication to his eye. His pupil gradually returned to size over the next 5 days, with complete return of visual and constrictive function.
DISCUSSION
The diagnosis of a pharmacological unilateral mydriasis can be inferred from the patient’s lack of ocular pain and ptosis, benign physical exam, and viable alternative explanation—exposure to a topical, anticholinergic medication.
Although the patient’s history of hypertension and unilateral mydriasis would be potentially concerning for a cerebral aneurysm, an otherwise benign neurologic examination makes this less likely. The patient had full range of his extraocular eye movements and the globe was not positioned in an inferior and abducted configuration, indicating that a cranial nerve three palsy from a possible aneurysm or tumor in unlikely. Additionally, he denies meningeal signs, seizure-like activity, or use of blood-thinning medication, making a hemorrhagic or ischemic stroke unlikely.
If a stroke did occur in the right cerebral hemisphere, the patient would also likely have a left lower facial droop and loss of movement and sensation on the left unilateral face, arm, and leg. Botulism is uncommon, and in addition to a benign neurological examination, there were no systemic symptoms such as bilateral descending paralysis, dilated pupils, and ptosis, as well as trouble swallowing and breathing which are typically seen with botulism.
Adie’s syndrome is incongruent with this patient’s demographics and would present with a pupil that is slowly reactive to light and constricts with accommodation.
Stimulant drug intoxication has been a known source to cause a dilated pupillary response. Cocaine has been shown to cause a unilateral mydriasis. However, the patient denies drug use and subsequently had a normal heart rate and was not euphoric, hypervigilant, anxious, or experiencing chest pains, making cocaine intoxication unlikely.
Recent eye trauma or surgery can lead to anisocoria. Conversely, the patient denies any recent eye trauma or surgery, and there were subsequently no indicators of obvious ocular trauma.
Acute-angle closure glaucoma is a common pathology to see a dilated and fixed pupil, but the patient’s dilated eye was painless, no halos were observed in the patient’s visual field, and the patient did not have a headache, ruling out acute angle closure glaucoma as the diagnosis.
Hyperhidrosis
Hyperhidrosis is a condition characterized by the excess production of sweat from eccrine sweat glands. Nearly 5% of the U.S. population is affected by hyperhidrosis, with most cases being primarily idiopathic in etiology. This condition impacts a patient’s life in a variety of ways, including impairing daily functions and social and work interactions. In addition, patients are often embarrassed to discuss symptoms with a care provider. The most common area affected is the axilla, but craniofacial involvement occurs in up to 10% of patients.1 There are a number of beneficial therapies approved for the management of hyperhidrosis, including topical aluminum chloride, topical glycopyrrolate, iontophoresis, botulinum toxin injections, and oral anticholinergic drugs. Selection of treatment regimen depends on severity and site involvement.2
Pharmacologic Agents Which May Cause Unilateral Mydriasis
There are several other pharmacologic agents that can cause a unilateral dilated pupil, such as:
- Parasympatholytic drugs (atropine, homatropine, tropicamide, cyclopentolate)
- Sympathomimetics (phenylephrine, clonidine, apraclonidine, brimonidine)
- Scopolamine patch for motion sickness, aerosolized anticholinergic drugs (ipratropium)
- Certain plants (jimsonweed)8
Of importance to note, unilateral mydriasis caused by a pharmacological etiology is not associated with pain, a drooping eyelid, or double-vision, consistent with the presentation of this patient.8 Additionally, the pharmacologic agent causing the anisocoria can be narrowed down by assessing the amount of dilation of the abnormal pupil.8 For instance, an anticholinergic drugs will cause >8 mm dilation and does not react to light, and a sympathomimetic drug will cause a 1-2 mm dilation.8
Glycopyrronium tosylate (Qbrexza) is a synthetic anticholinergic agent approved for the treatment of primary axillary hyperhidrosis. It is available in the form of a premoistened wipe to use on the underarm, once daily. Although the drug is only approved for primary axillary hyperhidrosis, it has been found to be safe and effective in reducing excessive facial perspiration as well. Because the drug is rarely absorbed systemically and is unable to easily cross the blood-brain barrier, adverse reactions are often mild and the result of peripheral anticholinergic activity.3 While dry mouth is the most commonly reported adverse event, more worrisome side effects such as mydriasis, blurry vision, and dehydration have also been reported.4
The time it takes for these adverse reactions to appear, as well as disappear, leads to a highly variable clinical picture once the drug is absorbed systemically. These findings explain the approximate 2-hour onset of action that was seen in our patient. In addition, the elimination pharmacokinetics likely account for why the mydriasis seen in our patient appeared to linger. This notion is supported in that the mean terminal elimination half-life depends on the route of administration: 2.8 hours after oral administration, 6.2 hours after intravenous administration, and 33 to 53 hours after inhalation.5
Recommendations
Unilateral mydriasis is a particularly alarming side effect, as it is frequently associated with a more life-threatening condition such as cerebral aneurysm or intracranial hemorrhage. The diagnostic approach in a patient with an isolated cranial nerve palsy should start with considering the age and medical comorbidities of the patient. If an aneurysm is suspected, then an MRI is indicated.10 The confusion of this side effect with a more serious condition has not only resulted in misdiagnoses, but also exposure to unnecessary neuroimaging and added medical costs.6,7
This case emphasizes the importance of obtaining a thorough history and physical exam, in addition to a detailed medication review, including topical medication to help avoid such outcomes. Patient counseling for this medication should stress the importance of proper hand washing after use and avoiding touching the area of application. Patient education pertaining to such side effects can allow for early identification that avoids added stress and costs for all parties involved.
References
- Nawrocki S, Cha J. The etiology, diagnosis, and management of hyperhidrosis: A comprehensive review: etiology and clinical work-up. J Am Acad Dermatol. 2019;81(3):657-666.
- McConaghy JR, Fosselman D. Hyperhidrosis: management options. Am Fam Physician. 2018;97(11):729-734.
- DailyMed. Drug label information: Qbrexza—glycopyrronium cloth. Available at: https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=6b985380-1256-4fb3-b89a-6df2c6a6d12e. Accessed January 29, 2019.
- Nwannunu CE, Limmer AL, Coleman K, et al. Glycopyrronium tosylate (Qbrexza) for hyperhidrosis. Skin Therapy Lett. 2019;24(2):1-3.
- Chabicovsky M, Winkler S, Soeberdt M, Kilic A, et al. Pharmacology, toxicology and clinical safety of glycopyrrolate. Toxicol Appl Pharmacol. 2019;370:154-169.
- Panting KJ, Alkali AS, Newman WD, Sharpe GR. Dilated pupils caused by topical glycopyrrolate for hyperhidrosis. Br J Dermatol. 2008;158(1):187-188.
- Al-Holou SN, Lipsky SN, Wasserman BN. Don’t sweat the blown pupil: anisocoria in patients using Qbrexza. Ophthalmology. 2020;127(10):1381.
- Kedar S, Biousse V, Newman N. Approach to the patient with anisocoria. UpToDate. Available at: https://www.uptodate.com/contents/approach-to-the-patient-with-anisocoria?search=unilateral%20mydriasis&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1#H18. Published May 28, 2019. Accessed March 9, 2021.
- Nelson L, Odujebe O. Cocaine: Acute intoxication. UpToDate. Available at: https://www.uptodate.com//contents/cocaine-acute-intoxication?search=unilateral%20dilated%20pupil&source=search_result&selectedTitle=6~150&usage_type=default&display_rank=6. Published January 11, 2019. Accessed March 8, 2021.
- Lee A. Third cranial nerve (oculomotor nerve) palsy in adults. UpToDate. Available at: https://www.uptodate.com/contents/third-cranial-nerve-oculomotor-nerve-palsy-in-adults?search=unilateral%20mydriasis&source=search_result&selectedTitle=2~150&usage_type=default&display_rank=2#H14. Published June 19, 2017. Accessed March 9, 2021.
Author affiliations: Kayla Penny, BS, Louisiana State University Health Shreveport, School of Medicine; Joseph LaRochelle, PharmD, BCPPS, FCCP, Xavier University of Louisiana, College of Pharmacy. Deirdre Hooper, MD, Louisiana State University Health New Orleans, Department of Dermatology; Haley Caire, BS, Louisiana State University Health Shreveport, School of Medicine; Kelsey Rooney, BS, Louisiana State University Health Shreveport, School of Medicine.

Kayla Penny, BS

Deirdre Hooper, MD

Haley Caire, BS

Joseph LaRochelle, PharmD, BCPPS, FCCP
