Published on
Urgent message: Patients with seemingly unusual conditions do present to urgent care, underscoring the need to always take a thorough history for all “red flag” symptoms.
LEE A. RESNICK, MD, FAAFP
Introduction
While the incidence of acute rheumatic fever has declined significantly in developed countries over the last several decades, sporadic cases do still occur. Diagnosis may be difficult due to the non-specific symptoms and the lack of experience with the condition amongst most urgent care practitioners. However, delays in diagnosis can lead to severe complications and even death, so urgent care providers must remain vigilant with a high index of suspicion. A refresher on the red flags and diagnostic criteria of acute rheumatic fever can help the physician identify at-risk patients who need further testing and evaluation. This case report highlights the presentation and its relevance to urgent care practice.
Case Presentation
An 18-year-old male presented to the urgent care with fever, sore throat and body aches of 2 to 3 days duration. Prior to entering the room, the physician was notified that a rapid strep test was completed per nursing protocol and was positive. The physician was relieved that he would be able to manage the encounter quickly within an otherwise busy Monday filled with other, more complex cases. The additional ease with which patient expectations can be met, through antibiotics and a quick recovery, makes this one of the most welcomed patient encounters in urgent care.
Confident, the physician entered the room for a requisite, though pre-rehearsed, History and Physical. Upon further questioning the patient explained, “Everything hurts: I have a headache, my body aches, I have chest pain…” He was nauseated over the weekend and had two episodes of emesis. He has been weak and febrile throughout the entire course. He revealed that he is a Division 1 offensive lineman on scholarship with a local university. His spring practices, the first of his Division 1 college career, start the following day, and he wanted to get treatment so he “doesn’t have to miss any practice time.”
Vital signs
- T: 101.5°F
- BP: 110/65
- P: 80 bpm
- O2 Sat: 99%
On physical exam, the patient looked moderately ill, but appropriate and typical for the diagnosis. He was a bit diaphoretic, but was also febrile. Vitals were otherwise normal. He was a large, athletic young man, consistent with his history. His tonsils were 2+, erythematous and full of exudate. The airway was patent and there was no sign of abscess. Neck exam revealed cervical adenopathy. Heart was normo-dynamic, and did not demonstrate any murmurs or gallups. There was no peripheral edema, no rash and no joint swelling or tenderness.
After leaving the room to write prescriptions, the physician became bothered by the “chest pain” comment from the patient. Although the examination did not reveal any cardiac signs, the physician felt compelled to inquire further. Upon further questioning, the patient clarified that the chest pain is different from the rest of the body aches. He stated the pain was constant, left sided and moderately severe in intensity. As the pain increased, the nausea and vomiting followed.
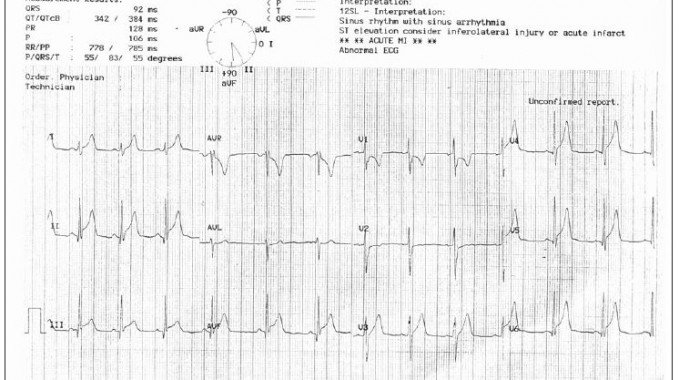
To the chagrin of the nursing staff, the physician ordered an electrocardiogram (EKG) and was shocked by the results. Diffuse ST elevations were present (Figure 1) consistent with carditis. While awaiting ambulance transfer, the patient was placed on O2 and a complete blood count and serum troponin test were ordered. The troponin I was 23.6 (reference range: 0.00-0.06). The patient’s WBC count was 11.4.
Disposition and Hospital Course
The patient was admitted to an academic medical center for further evaluation and treatment. An echocardiogram was performed which revealed severe LV dysfunction and an ejection fraction of 30% (less than half of normal for age). Cardiac magnetic resonance imaging (MRI) revealed diffuse myocarditis. The patient’s erythrocyte sedimentation rate (ESR) was very elevated, as was the Creactive protein (CRP). He patient was started on intravenous antibiotics and steroids. Interestingly, due to the rapid and acute nature of his presentation, his ASO titer was initially normal. In fact, ASO does not peak until 2 weeks after onset of symptoms, so a test that is initially negative does not rule out acute rheumatic fever. In a somewhat complicated course, this patient’s heart failure finally resolved and he was discharged 2 weeks later on high dose steroids that were to be continued for at least 6 months. He was given strict activity restrictions. His future in competitive athletics is unlikely.
Discussion
This is a dramatic case that could have ended very poorly. Considering the severe carditis and heart failure in this patient, had he returned to the practice field, he risked unimaginable morbidity and even mortality.
While acute rheumatic fever is thought of as a disease of developing countries, cases in the developed world still occur. It is noteworthy that cases in developed countries have a strong predilection for the upper class, a finding of unknown significance. The cases in the developed world also appear to be more acute and more aggressive, rising concerns that a virulent strain may be emerging. It has been theorized that high antibiotic usage rates in upper class communities may be contributing to these trends.
It is important to remember that most cases of acute rheumatic fever are preceded by a latent period of 1 to 5 weeks (mean of 18 days). Therefore, acute streptococcal pharyngitis is not usually present at diagnosis as it was in this case. Strep bacteria are only isolated in 25% of cases, and therefore, rapid antigen testing and throat culture are not reliable when negative (though positive tests are very helpful).
Diagnostic criteria have been revised over the years, but still use a version of the original Jones Criteria first noted in 1944. The diagnosis of acute rheumatic fever (first episode) is suggested by the presence of at least two major or one major and two minor criteria plus supportive evidence of previous streptococcal throat infection.
- Major criteria:
- Carditis (40%)
- Polyarthritis (80%)
- Chorea (rare)
- Subcutaneous nodule (<10%)
- Erythema marginatum (<10%)
- Minor criteria
- Fever
- Polyarthralgia
- Elevated ESR/CRP; leukocytosis
- Prolonged PR interval on EKG
- Supportive evidence of previous streptococcal throat infection:
- Elevated ASO and/or Anti DNAse B
- History of (within 45 days):
- Strep throat
- Scarlet fever
- Positive throat culture
- Positive rapid antigen test
Once the diagnosis is suspected, additional testing is suggested. Echocardiogram is a very useful tool for evaluating myocardial function and for identifying valvular involvement. Cardiac MRI is sometimes used to assess the extent of myocarditis.
Treatment with antibiotics and steroids is the mainstay of treatment, the details of which are beyond the scope of urgent care practice. Patients with carditis are at risk of developing rheumatic heart disease, therefore, steroids are often continued for extended periods (as in this case).
Conclusion
This case demonstrates that patients with seemingly rare or unlikely conditions do, in fact, present commonly in urgent care settings. It also serves as an important reminder to take a thorough history for all red flag symptoms in an “unbiased” way, without weight given to the time of day or business of the clinic. In this patient, the complaint of chest pain, while seemingly more likely to be a “constitutional” symptom of his strep throat, required its own history and confirmation of the physical exam. As it turns out, the decision to explore this symptom more thoroughly, and the concern that history revealed, was the difference in the outcome of this case.
References
- Digenea AS, Ayoub EM. Guidelines for the diagnosis of rheumatic fever: Jones criteria updates 1992. Circulation 87. Circulation. 1993;87:302.
- WHO Expert Consultation on Rheumatic Fever and Rheumatic Heart Disease (2001 : Geneva, Switzerland) Rheumatic fever and rheumatic heart disease : report of a WHO Expert Consultation, Geneva, 29 October — 1 November 2001.
Download the Article PDF: Acute Rheumatic Fever
