Published on
M.J. is a 12-year-old African American female who presented with trouble “taking a breath” which was abrupt in onset, starting two hours prior to presenting and accompanied with abdominal pain and fatigue which resolved prior to her visit. Dyspnea was constant and not related to position. There were no alleviating or aggravating factors.
Observations and Findings
Patient was alert and in no distress and spoke in full sentences. Pmhx: bronchitis one year prior; no asthma, no cardiac problems, no sickle cell disease
Meds: none
Social hx: no drugs or tobacco
Ros: no fever, lethargy, headaches, chest tightness, cough, wheezing, foreign body aspiration, abd pain, vomiting, back pain, dysuria, polyuria, polydipsia, rashes, swollen glands, extremity pain, falls, or injuries
Physical: t-98.7, p74, rr12, bp 98/60, o2 sat 97% ra
Resp: ctab no crackles or wheezes
Cor: rrr, no m/r/g were appreciated
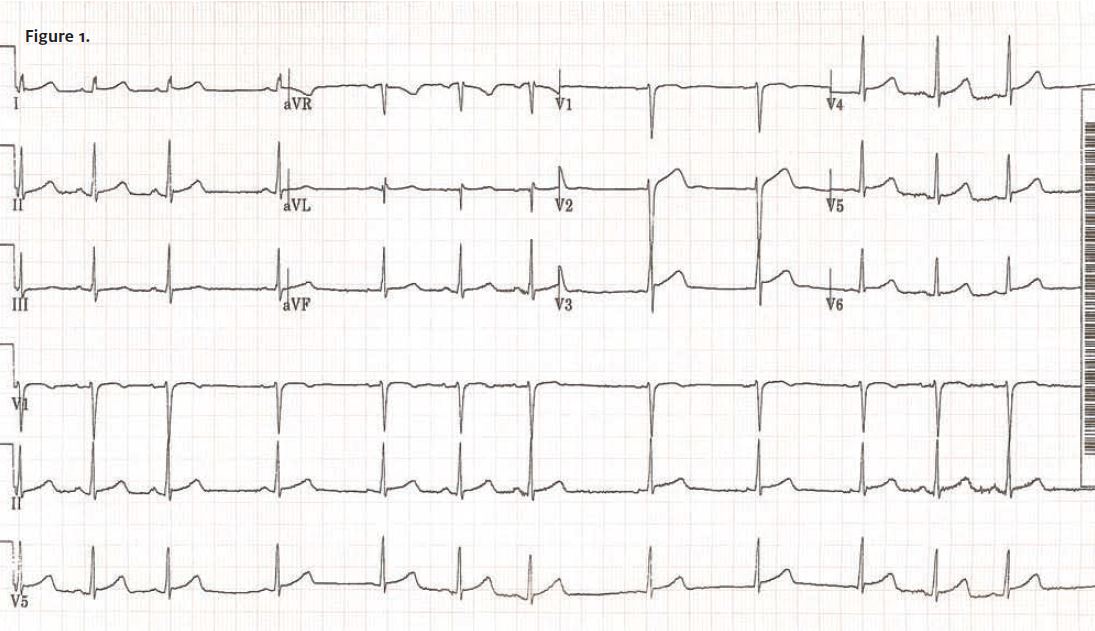
Diagnostic testing: CXR revealed a normal mediastinal silhouette, clear lung fields with no consolidation, effusion or pneumothorax. All other structures intact. EKG is shown for your review
(Figure 1).
Diagnosis
Acute pericarditis was determined by EKG, which reveals sinus rhythm with sinus arrhythmia, and diffuse ST segment elevation in at least two limb leads and all chest leads, especially v3-v6. Lastly, no ST-segment reciprocal changes, no Q-wave features, and T-waves are prominent and upright.
Discussion
Pericarditis is an acute or chronic inflammation of the pericardiinsights um. It is more common in males and most common in adolescents and young adults. Causes could include AMI or post-MI
(Dressler’s syndrome), be viral (coxsackie B, HIV) or bacterial in nature, or be related to collagen vascular disease, radiotherapy, local carcinoma, tuberculosis, uremia, or drugs (e.g., hydralazine, methyldopa, minoxidil, procainamide).
The most common type is fibrous and serofibrous occurring from AMI, uremia, radiation, RA, SLE, or trauma. Other types include serous, purulent, hemorrhagic and caseous.
Clinical signs: Pericardial friction rub: intermittent, positional best heard when sitting forward at the lower left sternal border, louder on inspiration. This can be difficult to detect and is present in approximately 50% of cases. Classical features of pericarditis are pericardial pain, friction rub, and a concordant ST elevation.
Differential diagnosis: Myocardial infarction, angina, aortic dissection, dyspepsia, pneumothorax.
Testing: EKG, CXR (useful to detect pneumothorax and pericardial effusion), PPD, HIV, ESR, CK, troponin (may be elevated in viral), ANA, RF, 2d-echo, CT/MRI.
Symptoms: Sharp, central, retrosternal precordial pain that is worse with deep inspiration, change in position, or exercise. May be sudden or gradual onset. May be relieved with sitting forward, or worse with lying back. Dyspnea is common, as are dry cough and dysphagia. Low-grade fever is a common finding. Patients could present with abdominal pain or just fatigue or malaise.
Treatment2006
Options range from no treatment with bed rest to anti-inflammatories (e.g., ibuprofen, indocin, prednisone), hospitalization (pericardiocentesis), or surgery (pericardiectomy), depending on age, severity and underlying cause.
Course of illness: Episodes may last one to three weeks; future episodes can occur. One in five people have recurrence within months of original episode. Repeated episodes may be treated with colchicine.
Possible complications include pericardial effusion and cardiac tamponade.\
Patient Course
M.J. was sent to the ER for further evaluation. An echo revealed no effusion. Initial workup labs were negative, and the patient was discharged home on NSAIDs with close follow-up. Of note: No instigating cause for this patient’s illness was found but a viral source is suspected.