Published on
Urgent message: Urgent care practitioners are called upon daily to alleviate pain. A thorough understanding of the various pain syndromes and the pharmacology and analgesic potencies of various medications will aid in their safe and appropriate use.
Marc R. Salzberg, MD, FACEP and Paolo T. Coppola, MD, FACEP
Pain, either chronic or acute, is the main reason patients seek medical care. In this article, we will discuss acute pain management in an urgent care setting, calling on over 30 years of collective experience in community emergency medicine and urgent care. For the purpose of this article, we will assume that the urgent care physician (UCP) has ordered and interpreted the correct labs and radiological studies, made the correct diagnosis, and has reviewed the patient’s allergy history and current medication usage. It is not the purpose of this article to address every possible pain syndrome. We will offer our strategies to effectively and correctly address the patient’s pain and expectations, while being mindful that meeting patients’ demand for pain medication may actually not be in the patient’s—nor the physician’s—best interest.
Rather, we will discuss analgesic equivalents, the appropriate and limited use of opioid medication, drug-seeking behavior (how to recognize it and what to do about it), and, finally, give several realcase scenarios that occur frequently in an urgent care setting. (It should be noted that many “pain management” physicians often prefer the term opioid to narcotic, as it has less of a negative connotation.
Technically, the terms are interchangeable, however.) Generally, it is the UCP’s responsibility to:
- Assess the quality and severity of
- Identify pain that may represent a medical or surgical
- Differentiate acute chronic pain.
- Assess pain that is the normal part of an injury or illness.
- Assess pain that may be the result of opioid depend- ence and its associated withdrawal
- Identify drug-seeking behavior
- Carefully document findings. (Remember the maxim, “In God we trust; all others must document.”)
Pain
Pain is an unpleasant sensory and emotional experience and is described as either nociceptive or neuropathic.
Nociceptive pain is the result of noxious stimuli that have the potential to damage normal tissue; it is either somatic or visceral. Neuropathic pain results from nerve lesions or another nervous system dysfunction and is either peripheral or central.
Pain is described by its quality, severity, location, and duration (chronic/acute). Some descriptors used to qual- ify the quality of pain include:
- sharp crampy • squeezing
- aching stabbing • burning
- throbbing knife-like • thunderclap
- pressure band-like • colicky
- tight dull • radiating
- electric burning • numbing
- tingling
Assessing Pain Severity
In addition to taking clues from the quality of a patient’s pain, the UCP must make a determination of its severity, as well. This can usually be done by simply asking a patient to rate his or her pain on a scale of 1-10. There are several pain scale measurement tools that are useful in assessing pain based on the patient’s perception. They include the visual analog scale (VAS) or numerical rating scale (NRS) for adults and the faces scale for children (Figure 1).
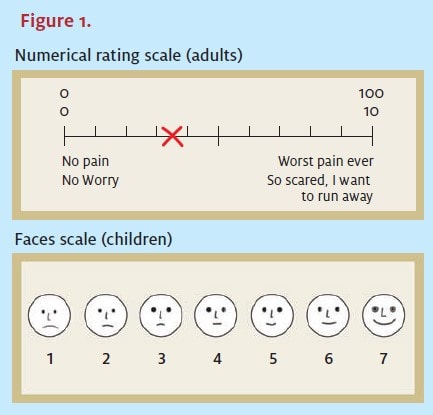
In addition, observation of the patient by the physician, nurses, and medical assistants can add to the clinical assessment. In an urgent care setting, quantifying the patient’s level of presenting pain, quality of pain, and response to your intervention should always be clearly documented and used to guide therapy.
Pain That May Represent a Medical/Surgical Emergency Clearly, pain sometimes is a warning sign of a true medical or surgical emergency. Classic examples in this category include, but are not limited to, the abrupt onset of “the worst headache of my life;” chest/- arm/neck/back pain that may represent an acute vascular process such as an acute MI, pulmonary embolism, or dissecting aneurysm; scrotal pain from testicular torsion; abdominal pain consistent with an intra-abdominal process such as appendicitis or diverticular abscess; abdominal pain out of proportion to physical findings as seen in mesenteric vascular occlusion; and acute eye pain from acute angle glaucoma.
Such presentations should be transported without delay to the nearest emergency department.
Acute Pain
Acute pain is pain that started abruptly or has increased over a short period (minutes to hours) and is ongoing (or intermittent and recurring, such as in renal colic). Examples of acute pain include trauma/burns, visceral/somatic pain such as abdominal pain, chest pain, acute gout, headache, eye pain, etc., and pain associated with an illness such as pharyngitis, urinary tract infections, influenza, and acute otitis media and externa.
Chronic Pain
Chronic pain, as the name implies, is a pain syndrome that has been ongoing. Examples may include discogenic pain, post-herpetic neuralgia lasting at least three months, pain from metastatic disease, chronic/stable angina, and chronic headaches (migraine, tension, etc.). Other chronic pain syndromes such as fibromyalgia and pain from chronic Lyme disease are more difficult to quantify, although often patients will present to urgent care centers with one of these diagnoses.
Fibromyalgia has been considered by some to be a “wastebasket” diagnosis for unexplained pain, and although the American College of Rheumatology established strict criteria for its diagnosis, in our experience only a small percentage of patients who have been so diagnosed actually meet these criteria. These and other chronic pain syndromes require a multidisciplinary approach and are not the purview of this article.
Pain Medication
Selection of the correct analgesic for a patient is based on the patient’s level of pain, the cause of that pain, prior medical history, current medications, other presenting complaints or comorbid conditions, vital signs, and the clinician’s assessment of the patient. It is also important to set realistic pain management goals so that someone with fractured ribs, for example, understands that the discomfort will take several weeks to improve. Although we will not address specific pain-relieving therapies such as trigger point injections or nerve blocks, they should be considered if you are familiar with and have experience in these modalities.
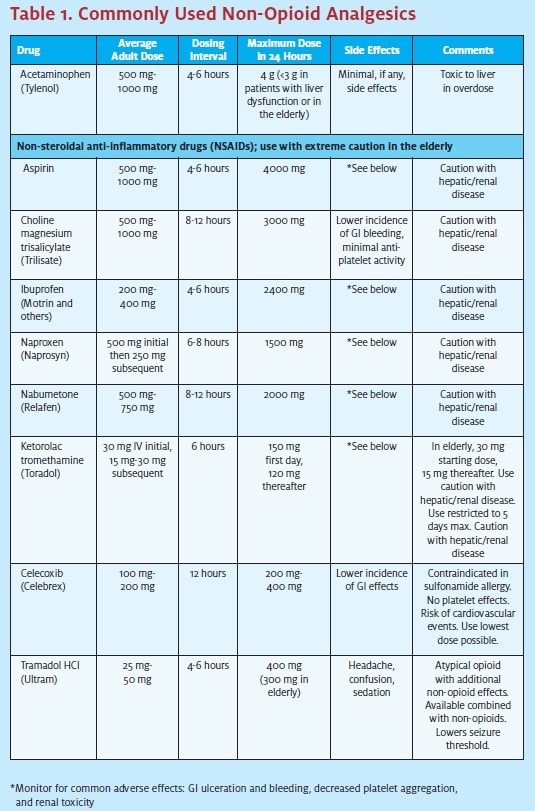
In general, most pain can be effectively managed with acetaminophen or nonsteroidal anti-inflammatory drugs (NSAIDs) or a combination of both, as they act synergistically when combined. Occasionally, a short course of oral opiates is warranted.
Non-Opioid Analgesics
Non-opioid analgesics include aspirin and other salicylates, acetaminophen, and NSAIDs. In general, non-opioid drugs are used to treat mild-to-moderate pain and in combination with opioids for more severe pain. Since opioids and non-opioids have different mechanisms of action, they can be used together to produce a synergistic effect.
Acetaminophen
Acetaminophen produces its analgesic effect by inhibiting central prostaglandin synthesis with minimal inhibition of peripheral prostaglandin synthesis. Prostaglandins are involved in sensitization of peripheral and central nociceptors, as well as in the inflammatory process.
Acetaminophen does not have an anti- inflammatory effect; nor does it have an adverse effect on platelet function or the gastric mucosa. It is rapidly absorbed, with peak plasma levels seen in 30 to 60 min- utes, and is metabolized in the liver by conjugation and hydroxylation to inactive metabolites.
Because of the risk of hepatotoxicity, acetaminophen should be used cautiously in patients with liver disease, chronic alcoholism, and malnutrition. As acetaminophen is readily available either alone or in combination with other drugs, recommended doses are often overlooked and must be followed to avoid a toxic overdose.
NSAIDs
NSAIDs act by inhibiting both central and peripheral prostaglandin synthesis. Inhibiting cyclooxygenase activity results in prostaglandin synthesis being blocked, thereby decreasing the inflammatory response.
NSAIDs block the production of prostaglandins but do not inhibit the effects of prostaglandins already present.
Therefore, although anti-inflammatory effects are relatively delayed, the anal- gesic effects occur more quickly. Respons- es to various NSAIDs vary among patients, so inadequate pain relief from one NSAID should not preclude the use of other drugs in this class.
NSAIDs are associated with GI effects including nausea, vomiting, and bleed- ing. Ketorolac has a slightly better pro- file for GI bleeding, but the risk is increased in elderly patients. Some physi- cians advocate the concomitant use of proton pump inhibitors or H2 blockers to lessen the GI effects of this class of drugs. Other adverse effects include nephrotoxicity, hepatotoxicity, and cognitive dysfunction.
Cyclooxygenase-2 (COX 2)-selective NSAIDs are effec- tive analgesics, but their role in pain management remains unclear in light of the serious safety issues that led to the withdrawal of rofecoxib and valdecoxib from the U.S. market, leaving only celecoxib available. There are also concerns about the increase in the international nor- malized ratio of patients being treated with both a COX- 2 inhibitor and warfarin. (See Table 1.)
Opioids
Opioids and related drugs are classified by their activity at different opioid receptors in the brain. The three main types of receptors that have been described are the mu, kappa, and delta; other receptors are thought to exist as well.
Mu receptor agonists produce analgesia and affect mood and behavior; delta agonists produce analgesia, although none of the currently available opioids are predominantly delta active; kappa-receptor agonists produce analgesia and relatively less respiratory depression but have psychological effects and can produce dysphoria.
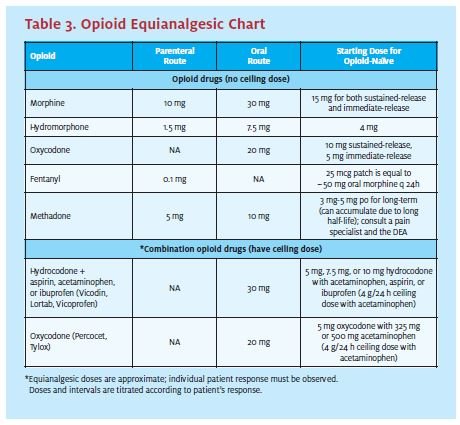
Table 2 is a list of opioids by receptor; Table 3 is an opioid equianalgesic chart.
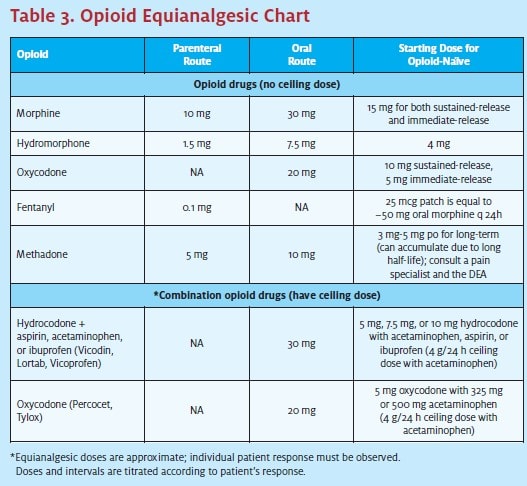
A few thoughts about narcotics: With very few exceptions, almost no patients presenting to an urgent care center require narcotics. If you feel that a patient does need an opioid drug (to treat renal colic, acute shingles, an acute fracture or burn, etc.), prescribe only one-to-two days worth and then have them switch over to an NSAID and/or acetaminophen. Any pain that requires more than two days of opioid medication must be re-evaluated for another serious underlying cause of the pain.
Some reasons/conditions for which you should not prescribe opiates include:
- “My pain doctor is away and I need a refill …”
- Low back pain—always assuming that you have made the correct diagnosis and it’s not an abdom- inal aortic aneurysm, Beware the patient who comes to you and says, “Here is my MRI showing my herniated L4/5.” In general, if the patient was able to get to you, he or she does not need nar- cotics. The overprescribing of narcotics for back pain is one of the leading causes of iatrogenic nar- cotic addiction.
- “I’m in withdrawal and I need something until….”
- “I have fibromyalgia, I’m from out-of-town and I need a refill of…”
- “Here’s the prescription from my last He’s in Antarctica now and I need….”
If you feel a short course (i.e., one to three days) of narcotics is appropriate, we recommend starting with the least addictive, such as tramadol (Ultram), and rapidly transitioning the patient to an NSAID and/or acetaminophen.
Because of the epidemic of prescription opiate drug abuse and addiction, we have made it a policy in our center to not write for more than two days of Vicodin, Percocet, or OxyContin, with no refills.
We are aware of some practitioners’ philosophy of “write them for the 60 Vicodin they want and get them out.” In our view, this is not only bad medicine but may end up costing you a substantial malpractice verdict. There have been numerous successful law suits against physicians for iatrogenic addiction.
An even more sobering thought is the fact that the DEA and other state agencies have been undertaking “sting” operations based on prescribing patterns of physicians.
ICDM 304.0: Opioid Dependence and Drug-Seeking Behavior
Patients who are opioid dependent often seek narcotics from urgent care centers, thinking they have more anonymity there than in a primary care office. Often, they are successful for all the wrong reasons. In an upcoming article, we will discuss in detail how you can help these patients treat their addiction with buprenorphine HCl/naloxone HCl (Suboxone), how to become certified by the DEA in its use, and how it can be beneficial to your practice.
Case Studies
Case #1
A 34-year-old female presents to your urgent care center complaining of two days of increasing dysuria, frequency, urgency, and lower abdominal cramps. Vital signs are normal and the patient is afebrile. Physical exam reveals only tenderness over the bladder with deep palpation. A urine analysis is positive for blood, nitrites, and leukocytes.
You prescribe an antibiotic and discharge the patient. A follow-up phone call two days later confirms that the infection is indeed resolved, but the conversation is marred by the patient’s complaint, “I went to my own doctor the next morning and he confirmed that I had a urinary tract infection and he shook his head that I was still in pain. He gave me Pyridium (phenazopyridine) and in 15 minutes all my discomfort was gone! What did you do for me?’’
Although this patient came to you to treat her UTI, she really came to you to treat her symptoms, as well.
Case #2
A 26-year-old male presents a half-hour after sustaining an inversion injury to his left ankle while playing basketball. On examination, he has normal vital signs, and neurovascular exam of his left lower extremity is normal. He has significant swelling over his left lateral malleolus. X-rays show soft-tissue swelling, but no fracture.
This patient’s pain and ankle sprain is best treated by:
- Immobilization of the ankle by an air- cast or other splinting device
- Non-weight bearing
- Crutches
- Ice and elevation of the ankle
- NSAIDs
- Referral to an orthopedist for follow-up care
The mainstay of treatment for this patient is immobilization and non-weight bearing. This will alleviate the majority of pain. The rest can be managed with NSAIDs along with acetaminophen. Opiates are not indicated.
Case #3
A 37-year-old woman presents to your office 15 minutes after cutting her left index finger with a knife while cutting a bagel. She is crying and scared.
After reassurance, you assess the wound for neurovas- cular compromise and tendon involvement and tell the patient she needs stitches and a tetanus booster. She wants to know how much it will hurt. You explain that the Lidocaine stings for a few seconds and that’s all. She screams loudly during the Lidocaine injection, after which the rest of your repair is painless.
At discharge she asks for pain medication for “after the Lidocaine wears off.” In fact, she mentions Vicodin, which she has been given in the past. Reassure the patient that when the Lidocaine wears off the pain will be minimal and that acetaminophen should take care of any discomfort. Any more severe pain would require a re- evaluation of the finger for infection, etc.
Case #4
A 27-year-old male presents complaining of severe low back pain for the past two days after helping a friend move furniture. He states that he has a ruptured disc at L4/5 and even has a copy of his last MRI report with him. On examination, his neurovascular exam is normal except for positive bilateral straight leg raising at 45 degrees. His urine is heme negative. Of note is his pulse of 120, BP of 145/98, and dilated pupils. He is afebrile. When you suggest a course of NSAIDs, he is quick to tell you that only Vicodin or OxyContin, which is “regular
doctor” prescribes, works for him.
It’s not possible to say he does not have low back pain, but it is clear that he presents a picture of narcotic withdrawal (specifically, tachycardia, dilated pupils, ele- vated blood pressure, and increasing back pain with his history of a ruptured disc). While these findings— with the exception of dilated pupils—can be consis- tent with severe pain, increasing bone and joint pain are classic symptoms of narcotic withdrawal.
We would recommend confronting this patient with your findings and suggesting that he needs treatment for his narcotic dependence. You can also do a toxicology screen on his urine, which you already collected.
Be aware that patients like this often become angry, abusive, and dismissive of your findings, then get up and leave. Be satisfied that you have done your job; hopeful- ly, you have planted a seed and he will eventually seek help for his narcotic dependence.
A practical note: In our center, patients presenting with back pain are given a policy statement that states we rarely prescribe narcotics for back pain, and if we do it will be for only one- to two days. We also have these patients pay for their visit prior to being seen.
Case #5
A 37-year-old women presents with two days of increasing right ear pain. Her past medical history is negative. Her vital signs are normal, as is her ENT exam, with the exception of a very red and swollen right external ear canal. The TM is normal. On further questioning, the patient states she uses cotton swabs (e.g., Q-tips) daily. For this patient, an ear-drop combination of an antibiotic and a steroid, such as ciprofloxacin/dexamethasone (Ciprodex), is indicated. A wick should be placed if the canal is so swollen that the drops would not go all the way in. A one- to two-day course of a combination opioid/NSAID is also appropriate.
In less severe cases, the drops and NSAIDs are usually sufficient. Follow-up is with ENT if there is not significant improvement in 24-36 hours.
Oral antibiotics are reserved for febrile patients in addition to the ear drops. And of course, remind the patient that “nothing goes in your ear unless it’s small- er than your elbow,” so no more cotton swabs.
Case #6
A 22-year-old male presents with two days of increasing throat pain, temperature to 101°F and a mild headache. Acetaminophen has offered no relief. Vital signs are normal, with the exception of an oral temperature of 101.5°F. ENT exam reveals a red pharynx, no exudates, normal tonsils, and no lymphadenopathy. A rapid strep test is positive. Penicillin is prescribed along with acetaminophen/NSAIDS.
Two days later, the patient returns with “unbearable” throat pain in spite of taking all the medication prescribed. He is afebrile and his ENT exam is unchanged. A three-day course of oral prednisone is given and on call- back the next day, the patient is significantly improved. Barring contraindications, a short course of steroids for acute inflammatory conditions like this or acute tendonitis, gout, etc., can offer he significant relief.
Summary
The management of pain is based on the correct diagnosis of the underlying problem and its natural course, a thorough understanding of the different medications available, and the appropriate prescription for each individual patient. This, combined with patient education and open communication, will most often result in appropriate and successful pain management.
Resources for Further Information
- American Academy of Pain Management, www.aapaimmanage.org
- American Academy of Pain Medicine, www.painmed.org
- American Pain Foundation, painfoundation.org
- American Pain Society, www.ampainsoc
- DEA, usdoj.gov/dea
- Mayo Clinic Pain Management, mayoclinic.com/ findinformation/diseasesandconditions/index.cfm
- MedlinePlus Pain, www.nim.nih.gov/medlineplus/pain.htm
- National Institutes of Health Pain Consortium, http://painconsortium.nih.gov
- Tufts U School of Medicine Masters of Science in Pain Research,
- Tufts.edu/med/prep
- www.pain.com/

Marc R. Salzberg, MD, FACEP
