Published on
Differential diagnosis:
- First-degree AV block
- Multifocal atrial tachycardia
- Wolff-Parkinson-White syndrome (WPW)
- Sinus bradycardia
- Third-degree heart block
Diagnosis
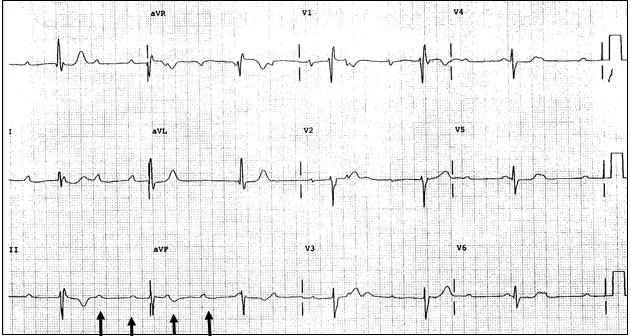
This patient has a third-degree AV block.
The first lesson in ECG interpretation is always to make sure there is a p wave preceding each QRS. This may not often be helpful, but when it is helpful, it is really helpful! This ECG reveals p waves and QRS complexes, but there is not a p preceding each QRS. Curiously, the p waves present are regular (see arrows below the ECG), as are the QRS complexes; they are just not related. This is third-degree heart block. Another clue is the rate, in the high 30s—an unusually slow bradycardia, even in a fit athlete.
The normal PR interval is 120–200 ms, with first-degree AV block a duration longer than 200 ms, but as there is not a defined PR interval, this is not first-degree AV block. Multifocal atrial tachycardia (MAT) is a tachycardia with a rate >100 beats per minute, and secondly is “multifocal” with differing P wave morphology; however, there is a p wave before each QRS, not present in this ECG. The ECG of WPW reveals a gradual upsloping of the initial reflection of the QRS complex (the delta wave usually seen in the lateral precordial leads), as well as a shortened PR interval (<120 ms), a widened QRS complex, and ST/T wave changes—not present on this ECG. Sinus bradycardia is a sinus rhythm <60 beats per minute. This rate is bradycardic, but is not sinus; this ECG shows third-degree AV block.
Learnings/What to Look for
- Third-degree AV block has complete absence of AV conduction. There is no relation of the p waves and the QRS complexes
- The rate of the atrial depolarization (p waves) is different than the ventricular rate
- The ventricular rate is often in the mid to high 30s
- Third-degree block may degenerate into cardiac arrest and death
- Potential causes include AV blocking medications such as beta blockers, calcium channel blockers, digoxin and amiodarone, electrolyte abnormalities, degeneration of the conducting system, or ischemia
Pearls for Urgent Care Management and Considerations for Transfer
- All patients presenting to the urgent care in third-degree heart block will need emergent transfer per EMS to the emergency department
- If symptomatic in the urgent care, atropine may be tried, but is not commonly successful
- Do not give atropine while awaiting transfer if the patient is asymptomatic
- If the patient is hemodynamically unstable place an IV and monitor, inform EMS for emergent transfer, and speak with the receiving facility