Published on
Differential Diagnosis
Normal sinus rhythm
Sinus bradycardia
Anterior ischemia
Junctional rhythm due to Hyperkalemia
Complete heart block
Diagnosis
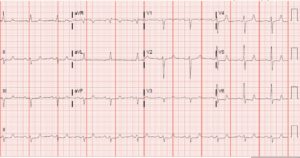
This patient was diagnosed with hyperkalemia. This ECG shows a rate of 42 BPM, which is bradycardic. There are no discernable P waves, and the typical junctional rate is between 40 and 60 BPM, so this is consistent with a junctional rhythm. Additionally, notice that the T waves appear peaked, a sign of hyperkalemia. These should be differentiated from tall hyperacute T waves of ischemia, which produce a broader base.
Hyperkalemia can cause many electrocardiographic changes, but hyperacute T waves, absence or flattening of P waves, bradycardia, and QRS widening are a few.
Case Resolution
This patient’s potassium returned at 7.9 meq/L. He was treated with 4 g IV calcium gluconate, 10 mg albuterol, and 5 units of insulin with an ampule of D50W—after which the following ECG was obtained:
(Note that in the post-treatment ECG, P waves have appeared, the rate is faster, and the QRS is narrower.)
Hyperkalemia is a cardiac membrane destabilizer, and recognition of its electrocardiographic findings is paramount to avoid deterioration into a more unstable rhythm like complete heart block or ventricular fibrillation. Three electrocardiographic findings have been demonstrated to predict short-term adverse outcomes: bradycardia <50 BPM, QRS widening >110 msec, and the presence of a junctional rhythm.
This patient’s ECG demonstrated all three. Classic electrocardiographic changes are shown in the following table, but it important to recognize that hyperkalemia is implicated in all kinds of electrocardiographic changes (not limited to those in the table).
| Serum Potassium | Potential ECG Changes |
| 5.5-6.5 mEq/L | Tall, peaked T waves with narrow base
QT interval shortening ST-segment depression |
| 6.5-8.0 mEq/L | Peaked T waves
PR-interval prolongation P wave decreased amplitude or disappearance QRS widening R-wave amplification |
| > 8.0 mEq/L | P-wave absence
QRS widening Intraventricular/fascicular/bundle branch blocks Sine wave |
Learnings/What to Look for
- Always obtain an ECG if hyperkalemia is suspected (i.e. when dialysis is missed)
- Typical electrocardiographic findings of hyperkalemia include peaked T waves, flattening or absent P waves, and QRS widening
- If unrecognized and untreated, hyperkalemia can deteriorate into ventricular fibrillation
- Three electrocardiographic findings predict short-term adverse events – bradycardia < 50 BPM, QRS widening >110 msec
Pearls for Urgent Care Management and Considerations for Transfer
- Hyperkalemia can be treated with membrane stabilizers like intravenous calcium gluconate (or calcium chloride if unstable), potassium shifters like beta agonists and insulin, and potassium excreters like furosemide and oral polystyrene sulfonate
- Patients with hyperkalemia should be transferred to an emergency department for consideration of emergent dialysis, but if resources are available, consider the above treatments prior to transfer
Acknowledgment: Images and case provided by Benjamin Cooper, MD, FACEP, assistant professor and associate program director, McGovern Medical School, Department of Emergency Medicine, The University of Texas Health Science Center at Houston.
