Published on
Urgent message: Injuries sustained in playground falls are common presentations to emergency departments and urgent care centers alike. The urgent care physician should be alert to the keys to evaluation and management of traumatic neck pain.
Muhammad Waseem, MD, Lalithambal Venugopalan, MD, and Gerard Devas, MD Cervical spine (C-spine) injuries occur infrequently in children. This is especially true for fractures of atlas vertebra, which is a rare injury in children. Its diagnosis may easily be missed due to inconclusive C-spine radiographs and absence of neurological signs. Here, the authors present an illustrative case of a patient with, and a review of, a fracture of atlas vertebra.
Case
A 4-year-old presented with neck pain one day after he fell from a slide onto the top of his head. He was complaining of pain in the back of his neck. There was no history of loss of consciousness, headache, or vomit- ing. He was immediately placed in a rigid cervical collar. In the emergency department, he was alert and awake.
His Glasgow coma scale was 15. His vital signs were as follows:
Temperature: 98.4°F
Heart rate: 119 beats/minute
Respiration: 22 breaths/minute
Oxygen saturation: 99%
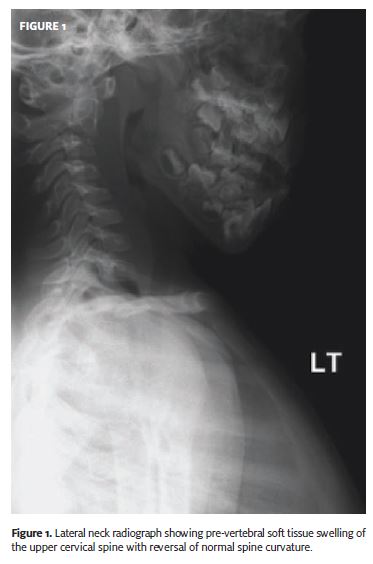
The patient did not have any difficulty of breathing but complained of diffuse neck pain. On physical examination, he had torticollis and diffuse tenderness over the back of his neck. There was no subcutaneous emphysema. The pupils were equal and reactive. There was no hemotympanum or cerebrospinal fluid leak from his ears. His chest was clear, with bilateral symmetric breath sounds. The abdomen was soft and non tender. His neurologic examination was unremarkable. Radiographs of the cervical spine (AP and lateral views done in erect posture) showed pre-vertebral soft tissue swelling of the upper cervical spine with reversal of normal spine curvature (Figure 1).
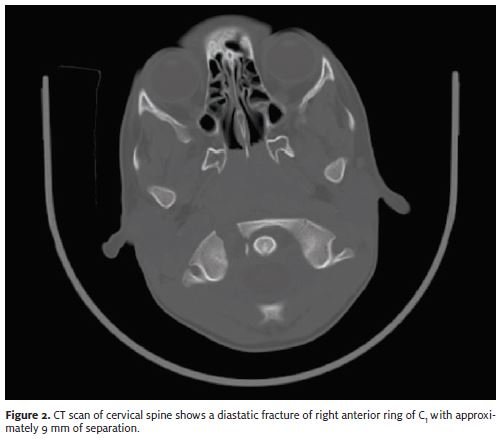
Because of the persistent pain and indirect signs of injury on the plain radiograph, a cervical collar was applied and the patient underwent computed tomography scan of the upper cervical spine, which showed a fracture in the right anterior arch of the C1 vertebra with a 9 mm separation (Figure 2). This fracture was considered stable and managed with immobilization. He improved and was well at follow-up.
Discussion
Cervical spine injuries are serious but relatively uncommon in children, with a reported incidence of 1% to 2%.1 The typical mechanism of cervical spine injury is either a fall onto the top of head or motor vehicle accident.
The fall onto the head causes the body weight to be transmitted to the atlas, resulting in axial loading.
Identification of the fractures of the cervical spine by plain radiograph is difficult and, there- fore, can be missed on plain radiographs.2,3 This is especially true for upper cervical vertebrae—including atlas, as most fractures of the atlas, particularly the anterior aspect, may remain occult.4
In addition, the open-mouth view, which is usually pathognomonic for the diagnosis, is often inadequate or not obtained.5 An open-mouth view is helpful to visualize the displacement of lat- eral masses of atlas, but may not demonstrate the site of fracture.
It is also important to look for any indirect signs of injury, such as pre-vertebral soft-tissue swelling, air in the pre-vertebral space, an increased width of the anterior atlantodental interval, and overriding of the C1-C2 joint on one side.6 Pres- ence of any indirect signs of injury on plain radi- ograph warrants a CT scan to confirm the presence of fracture of C-spine.
Younger children have a predilection for C- spine injuries at the higher level, which may be related to the biomechanical and anatomic features of the immature pediatric C-spine.7 The child’s spine is more flexible and mobile8 and, because of higher mobility and elasticity of the spine and a lower body mass in children, spinal injuries are relatively uncommon.9
It is especially rare in fractures of the atlas, as fracture of the ring increases the space that is available for the dural sac and, therefore, is unlikely to cause compression.10 Atlas fractures may be associated with other cervical fractures, with odontoid fracture being the most common associated fracture.
Management
The initial assessment of the patient must include maintenance of the airway, breathing, and circulation.
A non-displaced fracture of atlas is considered stable.11
Stable fractures usually heal with- in eight to 12 weeks.
Isolated stable fracture of the atlas can be treated effectively with a rigid cervical collar alone for that period.12 A Philadelphia collar may provide sufficient immobilization.
Generally, all displaced fractures are considered unstable; more rigid or surgical stabilization is recommended in unstable injuries in patients with displaced fractures.13 Another option is halo-vest immobilization for aperiod of 12 weeks.
Typically, cervical immobilization is sufficient for an isolated fracture of the atlas with an intact transverse atlantal ligament. However, cervical immobilization with surgical fixation and fusion will be required if transverse atlantal ligament is disrupted.14 The reported long-term outcome from the fracture of atlas is good.15
Disposition of Case
The patient described in this case report was treated conservatively with cervicothoracic brace; he recovered without any neurological abnormalities. In most reports, rigid collars, sternal occipital, mandibular immobilizer, or “SOMI”, braces and halo ring-vest orthoses have all been used for a period of eight to 12 weeks with good results. No evidence has been reported favoring use of one of these devices over the other.
Conclusion
It is important to consider fracture of the cervical spine in a child with significant neck pain and neck tilt after a fall on the top of the head. The presence of indirect signs of injury on plain films, especially in the presence of neck pain, should be taken seriously and followed with a CT scan.
REFERENCES
- Kokoska ER, Keller MS, Rallo MC, et Characteristics of pediatric cervical spine injuries. J Pediatr Surg. 2001;36:100-105
- Gale SC, Gracias VH, Reilly PM, et The inefficiency of plain radiography to evaluate the cervical spine after blunt trauma. J Trauma. 2005;59:1121-1125
- Besman A, Kaban J, Jacobs L, et False-negative plain cervical spine x-rays in blunt trauma. Am Surg. 2003;69:1010-1014
- Inaoka T, Ohashi K, El-Khoury A single fracture in the ring of vertebrae below the atlas: report of four cases. Emerg Radiol. 2007 Apr 24 [Epub ahead of print].
- Kesterson L, Benzel E, Orrison W, et Evaluation and treatment of atlas burst fractures (Jefferson frac- tures). J Neurosurg. 1991;75:213-220
- Ellis Imaging of the atlas (C1) and axis (C2). Emerg Med Clin North Am. 1991;9:719-732
- Finch GD, Barnes MJ. Major cervical spine injuries in children and J Pediatr Orthop. 1998;18:811–814.
- Akbarnia Pediatric spine fractures. Orthop Clin North Am. 1999;30:521-536.
- Patel JC, Tepas JJ 3rd, Mollitt DL, et al. Pediatric cervical spine injuries: defining the J Pediatr Surg. 2001;36:373-376.
- Levine AM, Edwards Fractures of the atlas. J Bone Joint Surg Am. 1991;73:680-691.
- Schlicke LH, Callahan A rational approach to burst fractures of the atlas. Clin Orthop Relat Res. 1981;154:18-21.
- Lee TT, Green BA, Petrin Treatment of stable burst fracture of the atlas ( Jefferson fracture) with rigid cervical collar. Spine. 1998;23:1963-1967.
- Kontautas E, Ambrozaitis KV, Kalesinskas RJ, et Management of acute traumatic atlas fractures. J Spinal Disord Tech. 2005;18:402-405.
- Congress of Neurological Surgeons. Guidelines for the management of acute cervical spine and spinal cord Isolated fractures of the atlas in adults. Neurosurgery. 2002;50 (3 Suppl):S120-S124.
- Hadley MN, Dickman CA, Browner CM, et Acute traumatic atlas fractures: Management and long term outcome. Neurosurgery. 1988;23:31-35.