Published on
The Resolution
Differential Diagnosis
- Groin sprain
- Lesser trochanter fracture
- Osteomyelitis
- Pubic rami fracture
- Septic arthritis
Diagnosis
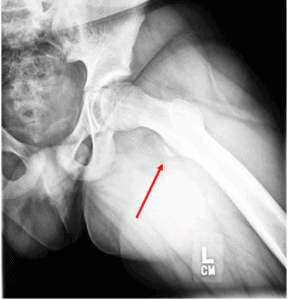
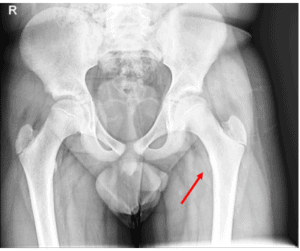
The x-rays reveal an acute Salter type I avulsion fracture of the lesser trochanter, with the nonvisualized lesser trochanter on the AP view of the pelvis and left hip and asymmetric widening of the lesser trochanter apophysis on the external rotation AP view. These fractures are typically associated with athletic activities in growing adolescents 13 to 17 years old with immature skeletons. It is common in skeletally immature soccer players from repetitive kicking motion with hip and knee in flexion.
Learnings/What to Look for
- Diagnosis is made on clinical, radiographic, CT, and MRI findings. An AP external rotation plain radiograph is needed for the diagnosis
- Clinical presentation includes a typical history of a specific athletic activity, localized pain, tenderness, limp, localized groin tenderness on palpation, and/or painful hip extension
- Radiographic findings include widened lesser trochanter apophysis and displaced lesser trochanter on AP external rotation view of the hip. The lesser trochanter may not be visible on AP views due to anterior displacement and overlap from the femoral cortex
- Isolated fractures of the lesser trochanter do not stem from the direct trauma, as the lesser trochanter is anatomically in a deep location and protected by large groin/thigh muscles and the femur itself. Rather, these fractures are usually from an indirect avulsion injury due to a sudden high-energy traction/pull of iliopsoas muscle on the femoral tendon insertion site
Pearls for Urgent Care Management and Considerations for Transfer
- Treatment is usually nonsurgical and includes rest in hip flexion, analgesics, and physical therapy
Acknowledgement: Images and case provided by Experity Teleradiology.
A 12-Year-Old Boy with Groin Pain
1 2