Published on
Case
The patient is a 45-year-old woman who presents after experiencing chest pain for the past 2 hours. She has some minimal dyspnea, but no diaphoresis. She takes birth control pills and is a smoker. She denies family history of cardiac disease.
Upon exam, you find:
General: Alert and oriented
Lungs: CTAB
Cardiovascular: RRR without murmur, rub, or gallop
Abdomen: Soft and NT without r/r/g
Ext: No peripheral edema or calf pain, pulses 2+ and equal in all extremities
View the ECG taken and consider what the diagnosis and next steps would be. Resolution of the case is described on the next page.
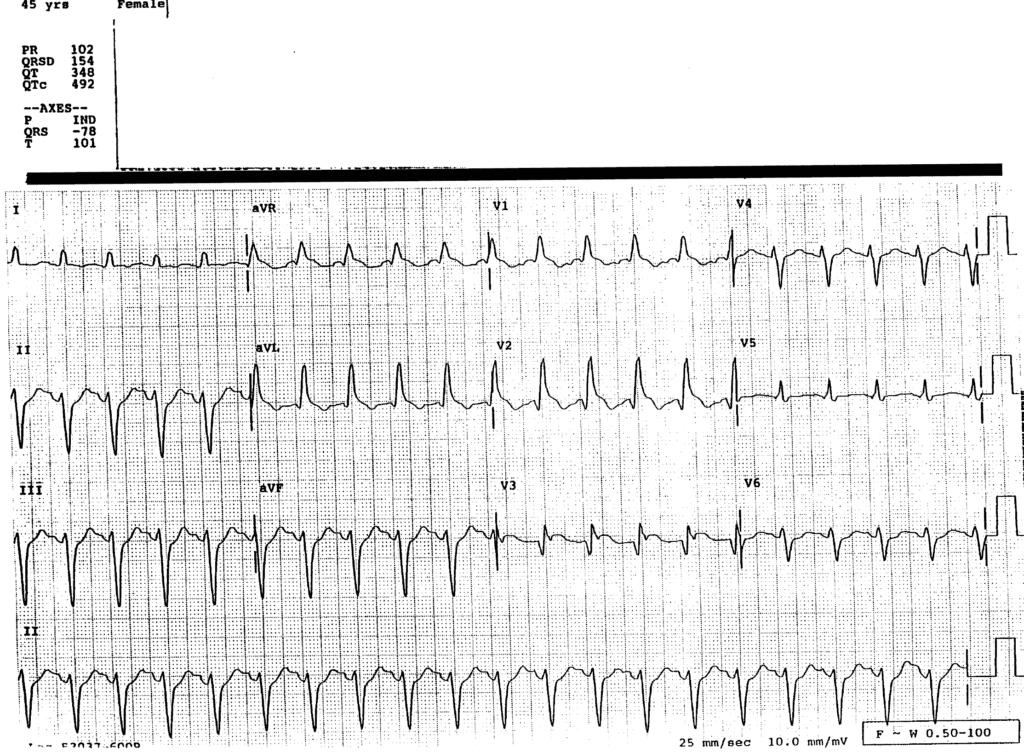
Figure 1.
A 45-Year-Old Woman with Acute Chest Pain
1 2