Published on
Download the article PDF: Clinical Image Challenges
Differential Diagnosis
- Second degree atrioventricular (AV) block (Mobitz type I) heart block
- Second degree AV block (Mobitz type II) heart block
- Posterior myocardial infarction (MI)
- deWinter T-waves
- Sinus bradycardia
Diagnosis
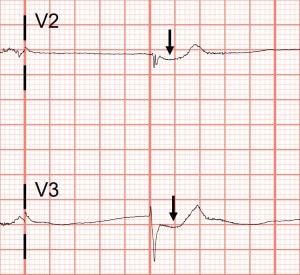
The correct diagnosis in this case is posterior myocardial infarction. The ECG shows a narrow complex, junctional bradycardia at a rate of 42. There are no discernible P waves (ruling out sinus bradycardia), and therefore no PR intervals (ruling out second degree AV block). There is focal ST-segment depression in V2 and V3, without ST-segment elevation elsewhere. The T-waves are not large in amplitude as expected with deWinter T-waves.
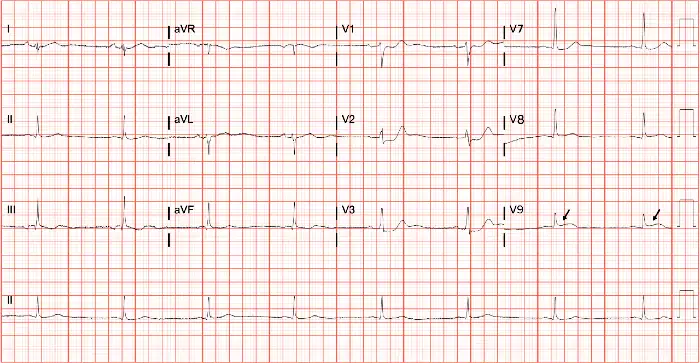
In the context of chest pain and anterior ST-segment depression, a posterior ECG should be performed on this patient by moving leads V4-V6 to the posterior chest wall, to better assess for posterior myocardial infarction (Figure 3).
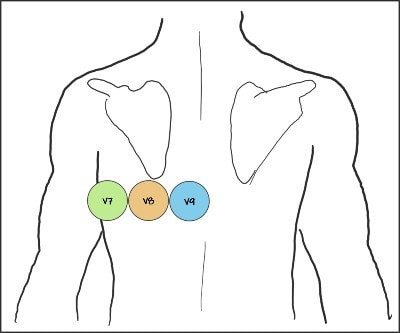
This patient was transferred to a percutaneous coronary intervention (PCI) center where an occluded proximal left circumflex was discovered and stented. The differential for ST-segment depression includes a broad range of conditions that can cause subendocardial (partial thickness) ischemia. The traditional 12-lead ECG does not contain leads that overly the posterior wall directly, therefore transmural infarction of the posterior wall is easily missed.1–3 By moving leads V4-V6 to the posterior chest wall to become V7-V9, you can distinguish between anterior subendocardial ischemia and posterior transmural infarction. Posterior myocardial infarction will show ST-segment elevation in V7, V8, and/or V9. Patients with posterior myocardial infarction require emergent intervention. Activate emergency medical services (EMS) immediately for transfer to a PCI-capable facility.4
What to Look For
- Isolated posterior myocardial infarction is a rare finding, occurring in 3-7% of acute MI, and likely underdiagnosed.
- Focal ST-segment depressions in the anterior leads may represent a posterior myocardial infarction.
- Consider an ECG with posterior leads when anterior ST-segment depression is noted.
Pearls For Initial Management, Considerations For Transfer
- Perform an ECG with posterior leads if you note focal ST-depressions in leads V1-4. Remember to relabel V7-V9.
- Activate EMS immediately.
- Administer aspirin (162-325 mg).
- After EMS activation and aspirin administration, establish IV access if able.
References
- Hähnle L, Viljoen C, Hoevelmann J, et al. Posterior infarction: a STEMI easily missed. Cardiovasc J Afr. 2020;31(6):331-334. doi:10.5830/CVJA-2020-059
- García-Arias MR, Salinas-Ulloa CY, Maravilla-Jiménez LR, Pinales-Salas R. Isolated posterior acute myocardial infarction: the responsible for subtle changes in the electrocardiogram. Arch Cardiol Mex. 2024;94(1):115-119. doi:10.24875/ACM.22000287
- Alsagaff MY, Amalia R, Dharmadjati BB, Appelman Y. Isolated posterior ST-elevation myocardial infarction: the necessity of routine 15-lead electrocardiography: a case series. J Med Case Rep. 2022;16(1). doi:10.1186/S13256-022-03570-W
- Kontos MC, de Lemos JA, Deitelzweig SB, et al. 2022 ACC Expert Consensus Decision Pathway on the Evaluation and Disposition of Acute Chest Pain in the Emergency Department: A Report of the American College of Cardiology Solution Set Oversight Committee. J Am Coll Cardiol. 2022;80(20):1925-1960. doi:10.1016/J.JACC.2022.08.750