Published on
Differential Diagnosis
- First-degree AV block
- Wolff-Parkinson-White
- Anterolateral ischemia
- Right bundle branch block
- Hyperkalemia
Diagnosis
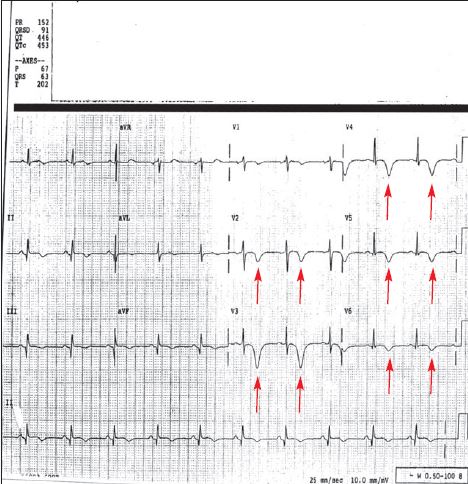
The patient has anterolateral ischemia. The ECG reveals T wave inversion, likely from ischemia, in the anterior and lateral distribution
Learnings/What to Look for:
- Leads V3 and V4 reflect blood supply to the anterior part of the heart, whereas leads I, aVL, V5 and V6 reflect blood supply to the lateral part of the heart
- The anterior part of the heart usually gets its blood supply from the left anterior descending artery (LAD), also called the “widow maker”
- The inferior part of the heart usually gets its blood supply from the right coronary artery (RCA). It is reflected on the ECG in leads II, III, and aVF
- Note that an isolated T wave inversion or Q wave in lead III only is a normal finding. (A Q is ‘free’ in III. A flipped T is ‘free’ in III)
Pearls for Urgent Care Management and Considerations for Transfer
- Compare to a previous ECG, if available, as anterior T wave inversions may also occur from intracranial processes, including bleeding
- Patients with chest discomfort and/or dyspnea with an ECG concerning for anterolateral ischemia should have emergent transfer to the ED. While awaiting transport, the patient should be monitored, have IV access obtained if possible, and receive 81-160 mg aspirin
- EMS should be notified that the patient has an ECG concerning for ischemia
A 51-Year-Old Man with Shortness of Breath and ‘Burning’ in His Chest
1 2