Published on
Differential Diagnosis
- Junctional Tachycardia
- First Degree Atrioventricular (AV) Block
- Hyperkalemia
- Second Degree Atrioventricular Block
- Sinus Arrhythmia
Diagnosis
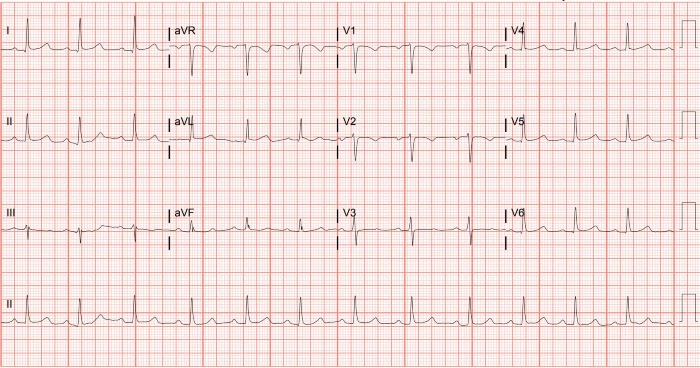
The diagnosis is first degree AV block. The ECG reveals a normal sinus rhythm with a rate of 72 beats per minute. The axis is normal. The PR interval is prolonged at 240 msec. There are no signs of ischemia.
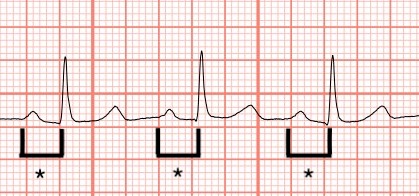
First degree AV block is a condition caused by an abnormally slowed conduction from atria to ventricles through the AV node. This is diagnosed on an ECG with a PR interval greater than 200 msec and is considered “marked” when the PR interval exceeds 300 msec.1 As seen in Figure 2, this interval is measured from start of the P wave to the beginning of the QRS complex. A normal PR interval is 120-200 msec.
First degree AV block can be caused by anything that slows the conduction from the atria to the ventricles. This includes AV nodal disease, enhanced vagal tone, ischemia such as inferior myocardial infarction, infection (eg, Lyme disease), inflammation, electrolyte abnormalities, and medications. Any medication that increases the refractory time of the AV node will slow the conduction through the AV node, such as calcium channel blockers, beta blockers, antiarrhythmics, and digoxin.2
In this patient’s ECG, the conduction to the ventricles is clearly slowed, but every atrial impulse is transmitted to the ventricles, in contrast to second or third-degree AV block. There are no other electrocardiographic abnormalities, making electrolyte abnormalities unlikely, and the rhythm appears to be regular, making sinus arrhythmia less likely. Classically, first-degree AV block, in isolation, is benign and asymptomatic, with no need for treatment or follow-up. However, if first degree AV block is seen in combination with other conduction deficits (eg, fascicular and/or bundle branch block), the patient is at higher risk of developing complete heart block. Therefore, recognition of first-degree AV block should prompt a focused history, physical, review of the patient’s medications, and comprehensive analysis of the ECG.
What to Look For
- First-degree AV block is diagnosed when the PR interval is longer than 200 msec and is often an incidental finding.
- In patients with first-degree AV block, look for additional signs of conduction delay on ECG and any other abnormalities such as ischemia or inferior myocardial infarction.
Pearls for Initial Management, Considerations For Transfer
- Typically, first-degree AV block is benign and requires no treatment or follow-up.
- If additional conduction deficits coexist, consider more advanced conduction system disease, assess hemodynamic status, and, if the clinical presentation warrants, consider transfer
References
- Ogunlade O, Akintomide AO, Ajayi OE, Eluwole OA. Marked First Degree Atrioventricular Block: an extremely prolonged PR interval associated with Atrioventricular Dissociation in a young Nigerian man with Pseudo-Pacemaker Syndrome: a case report. BMC Res Notes. 2014 Nov 4;7:781.
- Oldroyd SH, Quintanilla Rodriguez BS, Makaryus AN. First-Degree Heart Block. [Updated 2023 Jan 19]. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2023 Jan. https://www.ncbi.nlm.nih.gov/books/NBK448164/
Click Here to download the PDF