Published on
Differential Diagnosis
- Arrhythmogenic right ventricular cardiomyopathy (ARVC)
- Brugada syndrome
- Wellens syndrome
- Third degree heart block
- Wolf-Parkinson-White (WPW) syndrome
Diagnosis
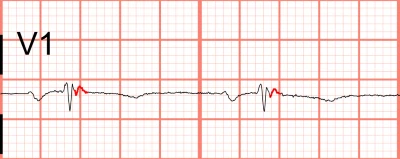
The diagnosis in this case is arrhythmogenic right ventricular cardiomyopathy. There is a normal sinus rhythm with a ventricular rate of 60 beats per minute, and there is an incomplete right bundle branch block pattern (iRBBB) in the right precordial leads (ie, V1 through V3) with associated T-wave inversions (typical for iRBBB). There is terminal notching of the QRS complex as seen in V1, which is consistent with Epsilon waves, confirming the diagnosis of ARVC.
Discussion
ARVC is an inherited and progressive condition characterized by structural abnormalities in the right ventricle that predispose it to ventricular arrhythmias and sudden cardiac death. The condition is more common in males, most prevalent in the Italian population, and usually discovered during adolescence.1,2 About 30% of patients will have Epsilon waves, which are terminal notches near the end of the QRS complex and are the most specific finding of ARVC.3 While Epsilon waves are a hallmark finding, they are a late finding of fatty and fibrous infiltration of ventricular myocardium and represent fragmented conduction through islands of surviving myocardium in the right ventricular outflow tract (Figure 2).
T wave inversions are the most sensitive finding, present in up to 85% of patients, and are generally found in the right precordial leads, as with our case.4 Other electrocardiographic findings include incomplete and complete right bundle branch block. Diagnosis is confirmed via magnetic resonance imaging, and treatment includes antiarrhythmics and implantable defibrillators.1 Patients with suspected ARVC should be referred to a center with electrophysiologic capabilities. The urgent care clinician should consider defibrillator pad placement prior to, and during, transfer.
Brugada syndrome is a sodium channel disorder and cause of sudden cardiac death; it is characterized electrocardiographically by a right bundle branch block appearance in V1 and/or V2 with coved-type ST-segment elevations.5 Wellens syndrome represents an ECG pattern seen in patients with critical stenosis of the proximal left anterior descending artery; it is characterized by biphasic T waves or deeply inverted, symmetric T waves in the anterior precordial leads.6 WPW is a ventricular pre-excitation syndrome that predisposes to arrhythmias.7 Electrocardiographic findings of WPW include a short PR segment, delta waves, and a slightly widened QRS—none of which are seen in this ECG. Additional electrocardiographic considerations for patients presenting with syncope include ischemia, heart blocks, hypertrophic cardiomyopathy, and prolonged QT.
What To Look For
- Arrhythmogenic right ventricular cardiomyopathy (ARVC) is a cause of sudden cardiac death, predominantly in young men
- It is characterized electrocardiographically by T wave inversions in the right precordial leads, and 30% may have Epsilon waves, terminal notches near the end of the QRS complex
Pearls For Initial Management, Considerations For Transfer
- Patients with suspected ARVC should be referred to an electrophysiologic center
- Place defibrillator pads while waiting for and during transfer
References
- Fontaine G, Gallais Y, Fornes P, Hébert JL, Frank R. Arrhythmogenic right ventricular dys-plasia/cardiomyopathy. Anesthesiology. 2001;95(1):250-254. doi:10.1097/00000542-200107000-00035
- Basso C, Corrado D, Marcus FI, Nava A, Thiene G. Arrhythmogenic right ventricular cardi-omyopathy. Lancet. 2009;373(9671):1289-1300. doi:10.1016/S0140-6736(09)60256-7
- Pérez-Riera AR, Barbosa-Barros R, Daminello-Raimundo R, et al. Epsilon wave: A review of historical aspects. Indian Pacing Electrophysiol J. 2019;19(2):63-67. doi:10.1016/J.IPEJ.2019.02.003
- T-Wave Inversions and Arrhythmogenic Right Ventricular Cardiomyopathy – American Col-lege of Cardiology. Accessed January 16, 2025. https://www.acc.org/latest-in-cardiology/articles/2019/05/16/16/28/t-wave-inversions-and-arrhythmogenic-right-ventricular-cardiomyopathy
- Brugada P, Brugada J. Right bundle branch block, persistent ST segment elevation and sud-den cardiac death: a distinct clinical and electrocardiographic syndrome. A multicenter report. J Am Coll Cardiol. 1992;20(6):1391-1396. doi:10.1016/0735-1097(92)90253-J
- de Zwaan C, Bär FWHM, Wellens HJJ. Characteristic electrocardiographic pattern indicat-ing a critical stenosis high in left anterior descending coronary artery in patients admitted because of impending myocardial infarction. Am Heart J. 1982;103(4 Pt 2):730-736. doi:10.1016/0002-8703(82)90480-X
Download the article PDF: 17-Year-Old With Syncope
