
Published on
Urgent message: Evaluating patients with acute scrotal pain can be a challenge for clinicians in the outpatient setting because several conditions indicated by it can cause significant morbidity. Performing a thorough but focused medical history and physical examination and considering certain diagnoses, including testicular torsion, epididymitis, and prostatitis, are imperative when assessing these patients.
JEREMY HAWKINS, MD, BRIT LONG, MD, and ALEX KOYFMAN, MD, FAAEM
Introduction
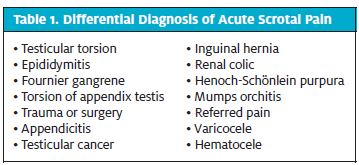
Evaluation of acute scrotal pain is often challenging for clinicians because of various overlapping clinical presentations from multiple disease processes. The precise epidemiology of acute scrotal pain in patients who pre sent for outpatient evaluation is largely unknown. The most critical component of evaluating all patients with acute scrotal pain is to promptly identify those who require emergency intervention. Lower genitourinary anatomy is important to understand when evaluating these patients. Structures that may be involved include the testis, appendix testis, tunica vaginalis, epididymis, spermatic cord, and prostate gland. The differential diagnosis of acute scrotal pain includes numerous conditions
Evaluation
Medical History
A detailed medical history and thorough physical examination are imperative in the evaluation and management of scrotal pain. When taking the medical history, health-care providers should query about the onset of symptoms (sudden vs. gradual), exact location of the pain, radiation, duration of pain (constant vs. intermittent), history of trauma or prior surgeries, and irritative urinary symptoms (frequency, urgency, dysuria, incomplete emptying of the bladder). The presence of abdominal pain or flank pain is also important when treating a patient with scrotal pain. Information on systemic symptoms such as fever, chills, nausea, vomiting, malaise, and weight loss should be elicited from the patient if they present. A focused past medical history must also be obtained to elicit a possible cause for scrotal pain, such as sexual activity, prolonged sitting, recent physical exertion, recurrent urinary tract infections, and recent instrumentation.
Examination
The clinician must perform a thorough genitourinary examination and examine the abdomen and flanks. The initial examination should begin with a general inspection of the groin and genitalia. If the patient is uncircumcised, external examination of the foreskin should be followed by reduction to completely expose the glans and allow visualization of any scars, ulcers, or other signs of inflammation. A small amount of whitish dis- charge under the foreskin can be normal. The urethral meatus should be gently opened to inspect for the presence of discharge. The scrotum must be inspected thoroughly, with the clinician taking note of any edema, erythema, induration, and abscesses. The scrotum should also be gently lifted to expose the posterior surface and the perineum to ensure that there are no signs of Fournier gangrene, such as crepitus, skin breakdown, or discoloration. Scrotal elevation during examination may alleviate some of the pain the patient is having (Prehn sign), indicating a pathology such as epididymitis that is less of an emergency, though this does not rule out testicular torsion. The most important aspect of examination is the testicles, because evaluation for testicular torsion must be at the forefront of the differential. The testis and epididymis must be palpated gently to evaluate the lie of each testicle (normal being longitudinal). Gentle palpation should not cause any discomfort if there is no pathologic process. The spermatic cord should be palpated, and any irregular nodules should be noted.1 It is also important to assess the cremasteric reflex by gently stroking or pinching the upper thigh. The ipsilateral testis normally elevates with cremasteric contraction during a normal response. When testicular torsion is present, the reflex is often absent.2 The clinician must evaluate for inguinal and femoral hernias, which may refer pain to the testis. If urinary symptoms are present with perineal or back pain, a rectal examination is warranted to evaluate for prostate enlargement, warmth, and tenderness. Examination for inguinal lymphadenopathy, suggestive of epididymitis or orchitis, and for costovertebral tenderness, a sign of pyelonephritis, is required. The most useful laboratory studies to obtain are urinalysis, urine culture, and gonorrhea and chlamydia studies. Color Doppler ultrasound (US) of the scrotum should be performed in any case where torsion is suspected, and a urologist should be consulted.
 Testicular Torsion
Testicular Torsion
Background
Testicular torsion is a twisting of the testicle along the longitudinal axis of the spermatic cord that can lead to ischemia of the testicle if treatment is delayed. Torsion is a urologic emergency. Although testicular torsion can occur in patients of any age, there is a bimodal peak in incidence, with most cases occurring in neonates and in adolescents around puberty. Torsion may be either intravaginal or extravaginal. Intravaginal torsion is due to a congenital anomaly called a bell clapper deformity, which allows the testicle to freely rotate within the tunica vaginalis. This occurs when there is a failure of the testicle to anchor posteriorly within the tunica vaginalis; it occurs more commonly in older children and adults. Extravaginal torsion occurs when there is inadequate fusion of the testicle to the scrotal wall, allowing rotation along the spermatic cord. This form presents in the post- natal period as painless testicular swelling. Both forms result in vascular congestion and decreased blood flow.
Presentation and Management
The classic presentation is sudden-onset, severe, unilateral scrotal pain. The pain is often associated with swelling, nausea, and vomiting. Many patients will report a recent history of trauma or significant strenuous activity. The classic physical examination findings include a high-riding testicle with a horizontal orientation and absence of the cremasteric reflex, though these are not definitive. The skin overlying the testicle may be warm, erythematous, and indurated. Intermittent torsion may result in recurrent painful episodes, with resolution between these episodes. Studies that should be obtained include a urinalysis and color Doppler US, with urologist consultation.3–5 Torsion of the testicle initially causes venous occlusion, and if it is persistent, it will ultimately lead to arterial occlusion, causing ischemia. Irreversible damage is thought to occur after 6 hours of ischemia. Findings on Doppler US may be normal in the early stages of torsion or in intermittent torsion. Initial changes seen on Doppler US are testicular enlargement and edema, which later give way to a heterogeneous and hyperechoic tissue appearance.6 A patient with a suspected testicular torsion should be transferred to the emergency department (ED) immediately for further evaluation and surgical consultation, because repair within 6 hours results in salvage rates approaching 100%. If the nearest ED is some distance away, manual detorsion may be attempted while preparing the patient for transfer; however, manual detorsion attempts should not delay transfer. Manual detorsion is achieved by twisting the affected testicle laterally. This is accomplished by outward rotation of the provider’s hands as if opening a book, with an end point of subjective decrease in pain. US should be used to confirm return of blood flow. Surgical intervention is still necessary even if detorsion is successful.3–5
Epididymitis and Orchitis
Background
Epididymitis and orchitis are common causes of acute scrotal pain that must be differentiated from testicular torsion. Epididymitis is more common than orchitis, which usually occurs because of a spread of the infection from the epididymis to the testes, which is considered epididymorchitis. In 2002, these two entities accounted for 1 in 144 visits in the outpatient setting in men between the ages of 18 and 50 years. Epididymitis occurs from retrograde ascent of pathogens, causing inflammation and infection. There are many causes of epididymitis, and these are usually differentiated on the basis of patient age. In this discussion, etiologies are limited to the most common causes.
In children younger than 13 years of age, the most common causes are postinfectious inflammatory reactions to entities such as enteroviruses, adenoviruses, and mumps. Sexually transmitted Neisseria gonorrhoeae or Chlamydia trachomatis are the most common causes in males 14 to 35 years of age. In men older than 35 years, infectious urinary pathogens such as Escherichia coli are the most likely cause of epididymitis; however, a detailed medical history, including information about sexual practices, must be obtained in this age group. Risk factors include sexual activity, prolonged sitting, recent instrumentation, and urinary tract abnormality. Immunocompromised patients and patients with human immunodeficiency virus are predisposed to fungal and viral etiologies. Other causes include medications such as amiodarone.
Presentation and Management
Patients usually present with gradual onset of pain that is isolated to the scrotum. Those with a more severe infection often present with scrotal swelling and pain as well as systemic symptoms such as fever, chills, and malaise. Severe infections are also more likely to be associated with irritative lower urinary tract symptoms like dysuria, frequency, urgency, and hematuria. The patient may present with nausea and vomiting, as in testicular torsion. Physical examination reveals a tender, swollen epididymis on palpation, mainly on the posterior scrotal aspect, and an intact cremasteric reflex. Tenderness isolated to the upper pole of the testis and relief of pain with scrotal elevation are both examination findings suggestive of epididymitis, though not diagnostic. Regional lymphadenopathy is also consistent with epididymitis. Costovertebral angle tenderness should be assessed to identify any associated pyelonephritis. Patients with severe systemic symptoms must be transferred to an ED for a more thorough evaluation. Urinalysis and urine culture should be obtained in all patients who present with symptoms that are concerning for epididymitis. Assays by polymerase chain reaction for N. gonorrhoeae and trachomatis are recommended for those patients considered at high risk for sexually transmitted infections (STIs). Cultures should be obtained of any discharge. Doppler US is often warranted to evaluate testicular blood flow, and it will reveal an enlarged, thickened epididymis with increased Doppler flow. Any suspicion of testicular torsion requires urology consultation.
Treatment should be directed at the most likely pathogen. Males between the ages of 14 and 35 years, as well as patients with a history of anal intercourse or in whom there is concern for STI, should be treated with a single dose of ceftriaxone (250 mg intramuscularly) and doxycycline (100 mg orally, twice daily) for 10 days. When coliform bacteria are suspected or the patient can- not take ceftriaxone or doxycycline, ofloxacin (300 mg orally, twice daily) or levofloxacin (750 mg orally, once daily) for 10 days should be used. Often overlooked, symptomatic treatment should also be recommended: nonsteroidal anti-inflammatory medications, scrotal elevation, and ice packs.7 Close outpatient follow-up will be required. Admission is warranted for intractable pain, vomiting, abscess formation, outpatient treatment failure, and sepsis. Orchitis treatment requires bed rest and hot or cold packs with nonsteroidal anti-inflammatory medications. Antibiotics are not required for most causes of orchitis; resolution usually occurs within 3 to 10 days. If a bacterial source is suspected, antibiotics are needed.7
Prostatitis
Background
Prostatitis is a clinical syndrome caused by inflammation and swelling of the prostate, with the potential to have drastic impact on quality of life. Prostatitis is one of the most common urologic complaints in men younger than 50 years of age and affects up to 16% of American men over the course of their lifetime. Prostatitis is categorized into four distinct clinical syndromes: acute bacterial prostatitis (type I), chronic bacterial prostatitis (type II), chronic pelvic pain syndrome (type III), and asymptomatic inflammation (type IV). Type III is the most common form, making up approximately 90% of diagnosed cases. Acute bacterial prostatitis and chronic bacterial prostatitis occur in only a small pro- portion of cases. Type II accounts for approximately 5% to 10% of patients with prostatitis. Type I accounts for the least number of cases, with < 1% of patients having an acute infection; however, acute bacterial prostatitis has the potential for significant morbidity and mortality.8 Risk factors for bacterial prostatitis include
 urinary tract infections, urethral strictures, instrumentation of the urinary tract, benign prostatic hyperplasia, and urethritis from STIs. The most common bacteria associated with acute and chronic prostatitis are E. coli, Klebsiella species, Proteus species, and Pseudomonas species; however, a significant number of chronic bacterial infections are attributed to C. trachomatis, Trichomonas vaginalis, and Ureaplasma urealyticum. These latter organisms are predominantly sexually transmit- ted, primarily affecting those younger than 35 years.4,5,7 This review focuses on the evaluation of acute and chronic bacterial prostatic infections.
urinary tract infections, urethral strictures, instrumentation of the urinary tract, benign prostatic hyperplasia, and urethritis from STIs. The most common bacteria associated with acute and chronic prostatitis are E. coli, Klebsiella species, Proteus species, and Pseudomonas species; however, a significant number of chronic bacterial infections are attributed to C. trachomatis, Trichomonas vaginalis, and Ureaplasma urealyticum. These latter organisms are predominantly sexually transmit- ted, primarily affecting those younger than 35 years.4,5,7 This review focuses on the evaluation of acute and chronic bacterial prostatic infections.
Presentation and Management
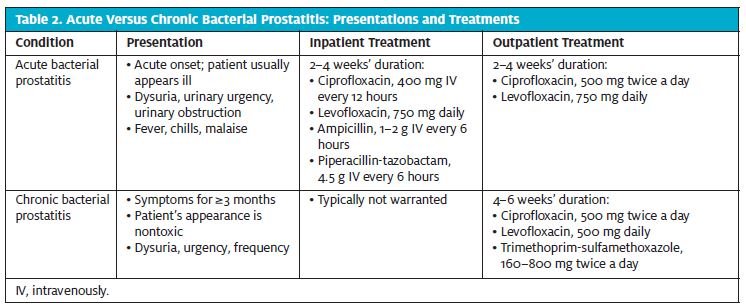
Table 2 summarizes the presentations and treatments for acute bacterial versus chronic bacterial prostatitis.
Acute Bacterial Prostatitis
Acute bacterial prostatitis typically presents with irritative or obstructive urinary symptoms with pain. Patients who have true acute bacterial prostatitis usually appear ill. Systemic symptoms of fever, chills, malaise, nausea, and vomiting may be present. Physical examination should include a digital rectal examination and an abdominal examination. Gentle palpation of the prostate should be performed, which may reveal an enlarged, tender, and boggy prostate. Prostatic massage should not be performed, because this can cause bacteremia and sepsis. Diagnosis of acute bacterial prostatitis requires the presence of polymorphonuclear leukocytes and bacteria in the urine.
Treatment should be initiated at the time of evaluation, and treatment choice should be based on whether thepatient appears acutely toxic. Any patient who appears acutely ill should be referred to an ED for further evaluation and management, because acute prostatitis can lead to prostatic abscess and epididymitis. If the patient is acutely ill or toxic, urology consultation is required, along with admission to an inpatient unit. Laboratory examination in these patients is required, including a complete blood count and a renal function panel. Concern for STI requires testing for likely agents. Initial empiric therapy for an acutely ill patient, if started prior to transfer to an ED, should be with ciprofloxacin (400 mg IV), levofloxacin (750 mg IV), ampicillin (1–2 g IV), or piperacillintazobactam (4.5 g IV). If bacterial resistance is suspected, a carbapenem such as ertapenem (1 g IV) or imipenem (500 mg IV) can be initiated if available. Patients who do not have a toxic appearance can be treated on an outpatient basis with oral antibiotics such as ciprofloxacin (500 mg twice a day) or levofloxacin (750 mg once daily). An alternate regimen includes trimethoprim-sulfamethoxazole double-strength (TMP-SMX DS), at 160 to 800 mg twice a day. Therapy for acute bacterial prostatitis should last 2 to 4 weeks.9,10
Chronic Bacterial Prostatitis
Chronic bacterial prostatitis typically presents with irritative urinary symptoms such as urgency, frequency, dysuria, penile or perineal pain, and lower back pain. Chronic infection should be suspected in those who have recurrent urinary tract infections and grow the same strains of bacteria on multiple separate cultures. Symptoms of irritation must be present for at least 3 months. Between episodes of prostatitis in the chronic form, patients often have no symptoms. Physical examination should include an examination of the lower abdomen and the genitalia as well as a digital rectal examination. The prostate may be tender, boggy, or indurated. A detailed examination should be completed to exclude anatomic abnormality of the urinary tract. The gold standard for diagnosis of chronic prostatitis is the four-glass test, but this is rarely used and is labor intensive. The two-glass test, used more frequently, is performed by comparing specimens from before and after prostatic massage.
Treatment with antibiotics in patients suspected to have chronic prostatitis can typically be delayed until culture results with sensitivities are obtained. Fluoroquinolones are the preferred initial therapy, with either ciprofloxacin (500 mg twice a day) or levofloxacin (500–750 mg once daily) unless antibiotic resistance is suspect- ed. Alternate regimens include TMP-SMX DS (1 tablet twice a day) or azithromycin (500 mg once daily). If STI is suspected, patients should be treated with ceftriaxone (250 mg intramuscularly for 1 dose) fol- lowed by doxycycline (100 mg twice a day). The duration of therapy should be 4 to 6 weeks.9,10
Chronic pelvic pain syndrome accounts for the majority of prostatitis, with patients experiencing long- term pelvic or perineal pain. Diagnosis is based on the amount of white blood cells found in prostatic secretions, semen, or urine after prostate massage.8–10
Conclusion
Patients presenting with acute scrotal pain can present a significant challenge for clinicians in the outpatient setting. Obtaining a thorough medical history, perform- ing a thorough but focused examination, and having a high clinical suspicion for certain diagnoses are imper- ative when evaluating scrotal pain. Any patient with a concerning medical history, disconcerting findings on physical examination, or a toxic appearance should be referred to an ED for further evaluation. When torsion is suspected or uncertain, urgent referral to an ED is indi- cated, with consultation with a urologist. Although conditions requiring urgent referral are relatively uncommon, clinicians will be far less likely to miss emergency conditions by maintaining a systematic, thorough approach and keeping emergency conditions in the differential diagnosis.
References
- Bickley LS, Szilagyi Male genitalia and hernias. In: Bickley LS, ed. Bates’ Guide to Physical Examination and History Taking. 9th edition. Philadelphia, PA: Lippincott, Williams & Wilkins; 2007:416–420.
- Caesar RE, Kaplan The incidence of the cremasteric reflex in normal boys. J Urol. 1994;152(2 pt 2):779–780.
- Sharp VJ, Kieran K, Arlen Testicular torsion: diagnosis, evaluation, and management. Am Fam Physician. 2013;88:835–840.
- Srinath Acute scrotal pain. Aust Fam Physician. 2013;42:790–792.
- Gordhan CG, Sadeghi-Nejad Scrotal pain: evaluation and management. Korean J Urol. 2015;56:3–11.
- Wright S, Hoffmann Emergency ultrasound of acute scrotal pain. Eur J Emerg Med 2015;22:2–9.
- Trojian TH, Lishnak TS, Heiman Epididymitis and orchitis: an overview. Am Fam Physi- cian. 2009;79:583–587.
- Benway BM, Moon Bacterial prostatitis. Urol Clin N Am. 2008;35:23–32.
- Videčnik Zorman J, Matičič M, Jeverica S, Smrkolj Diagnosis and treatment of bac- terial prostatitis. Acta Dermatovenerol Alp Pannonica Adriat. 2015;24:25–29.
- Lipsky BA, Byren I, Hoey Treatment of bacterial prostatitis. Clin Infect Dis. 2010;50:1641–1652.