Published on
Dianne Treacy Lore DNP, FNP-BC, CPNP-PC and Marlena Seibert Primeau DNP, FNP-BC, NHDP-BC, BSHEC
Citation: Lore DT, Primeau MS. Investigation and assessment of urine culture importance in the evaluation of uncomplicated urinary tract infections in an urgent care setting. J Urgent Care Med. 2021;16(2):37-41.
ABSTRACT
Purpose
Urinary tract infections negatively affect over 150 million individuals globally each year. Traditional management encompasses evaluating a urine culture and sensitivity (C&S). Although the guidelines set forth by the American College of Obstetricians and Gynecologists (ACOG) and the European Association of Urology recommend against the use of culture and sensitivity at the outset of treatment of an uncomplicated urinary tract infection, there is no formal policy in place at many primary care and urgent care clinics.
Population and Setting
The population parameters consisted of healthy, nonpregnant females 18 to 65 years of age who presented to the urgent care clinic with symptoms of dysuria. The setting was a suburban urgent care clinic in the southeastern United States.
Project Design
The project design consisted of the implementation of an evidence-based clinical practice guideline for quality improvement and development of a formal clinic policy in the treatment of uncomplicated urinary tract infections.
Evidenced-Based Procedure
The quality improvement project collected and analyzed data involving patients who presented with urinary symptoms consistent with a diagnosis of an uncomplicated urinary tract infection. The data were collected pre- and postintervention from the electronic medical record. Using the current ACOG evidence-based clinical practice guideline for the treatment of uncomplicated urinary tract infections as the foundation, a quality improvement clinical education presentation was provided to the providers of one urgent care clinic. The intervention was not ordering a urine culture and sensitivity on the selected population.
Evaluation
The outcome of this project was determined after the analysis of the pre- and postintervention data using a sample T-test.
Results
ACOG guideline application resulted in a 30% reduction in the ordering of a C&S in this population with no increase in the rate of follow-up needed in this postintervention group. The anticipated results supported the current ACOG clinical practice guideline and provide a basis for a formal policy in the urgent care setting.
Conclusion and Implications
Projects such as the one discussed in this article demonstrate that outcomes can be improved by promoting and implementing evidence-based clinical practice guidelines.
INTRODUCTION
Bacterial infections such as urinary tract infections (UTIs) negatively affect over 150 million individuals globally each year.1 A woman’s risk of acquiring a UTI is greater than a man’s due to their anatomical structure; the urethra of a female is both shorter and closer to the rectum than the male, increasing the risk of colonization of bacteria from the rectum. Other factors that place a female at increased risk for a UTI are sexual interaction, intercourse with a new partner, spermicidal use, poor hygiene, and history of UTIs as a child.2 The majority of the UTIs diagnosed annually are labeled as uncomplicated.2,3
An uncomplicated UTI is defined as an infection in the lower urinary tract among healthy, nonpregnant women with symptoms of burning upon urination, urinary urgency and/or frequency, and without the presence of flank pain, fever, vaginal pain, or discharge. The diagnosis of an uncomplicated UTI is made after a collection of subjective and objective data, including a thorough history of current symptoms, a physical examination, and the presence of leukocytes, blood, and/or nitrates on a urinalysis.2
Although characterized as having an “uncomplicated” UTI, many patients are negatively impacted by this condition. In the United States, UTIs constitute more than 10 million healthcare appointments with expenditures estimated to be over $1 billion annually.4 Uncomplicated UTIs affect both individuals and society due to losses in revenue and work hours. Approximately 70% of all adult women will acquire a UTI during their lifespan.4
Traditional management for an uncomplicated UTI encompasses evaluation of the results through use of a urine culture and sensitivity (C&S). A C&S provides key information such as the bacteria involved and the antibiotic appropriate in the management of an uncomplicated UTI.5 Conventional treatment of UTIs utilizes C&S testing to ensure that bacteria-to-drug mismatches don’t result in incomplete healing and necessitate return visits.
Although this has been the traditional standard of care, the American College of Obstetricians and Gynecologists (ACOG), the Centers for Disease Control (CDC) and the European Association of Urology (EAU) now recommend against the use of a C&S at the outset of treatment of uncomplicated UTIs.2,6,7 Since the bacteria E coli accounts for 75% to 95% of uncomplicated UTIs, a C&S does not alter the treatment or improve patient outcomes.8,9 According to Stapleton,9 a C&S should only be obtained for the diagnosis of complicated or recurrent UTIs.
Overall, laboratory tests can deliver valuable and lifesaving information for healthcare providers and are helpful in improving patient outcomes. When ordered appropriately, laboratory tests can assist directly in patient care and in the delivery of safe and affordable healthcare; however, when lab tests are ordered unnecessarily, these tests can add to the healthcare cost burden.10 According to Carroll,11 the Institute of Medicine reported that in 2013 over $200 billion was spent in America on “unnecessary services” such as superfluous laboratory tests.
The point-of-care testing (POCT) urinalysis, sometimes referred to as urine dip or dipstick, is a quick laboratory test performed onsite to detect substances in the urine sample.
It is a quick and inexpensive technique that is both sensitive (75%) and specific (82%) when searching for leukocytes or nitrates in urine.2 Per ACOG, the treatment of a symptomatic and uncomplicated UTI with leukocytes, blood, or nitrates noted on a POCT urinalysis does not require a C&S. A POCT urinalysis is a low-cost solution to contain healthcare expenses while providing quality patient care.2
METHODS
Over the past year, there has been increased discussion among providers at a university-affiliated urgent care clinic in North Carolina regarding the advantages and disadvantages of a C&S as part of the protocol for the treatment of uncomplicated UTIs. The debate between providers embodied the pros and cons of both approaches, as well as considerations of patient and provider time costs and ultimately the cost-effectiveness of the laboratory procedure.
A quality improvement project was developed to address this concern. Based on current ACOG clinical guidelines, the project’s goal was to ascertain the occurrence of unresolved UTI symptoms if C&S were not initially ordered for patients being treated for uncomplicated UTIs in healthy, adult nonpregnant females 18 to 65 years of age in an urgent care setting.
The urgent care clinic where the investigation took place is fast-paced and diverse, and an institution where patients visit for a myriad of urgent healthcare concerns throughout their lifespan. A substantial number of women within the target population present to this facility with UTI complaints. Based upon peer provider discussions, urine cultures represent a significant portion of the laboratory specimens obtained.
The population chosen for the project were healthy, nonpregnant females, 18 to 65 years of age, who presented to the urgent care setting with burning upon urination, urinary urgency and/or frequency, and possible blood, leukocytes, and nitrates identified in their POCT urinalysis results. However, these patients did not present with flank pain, fever, vaginal irritation, or discharge. The exclusion criteria were males, pregnant females, females with a history of recent UTIs, recent antibiotic use, diabetes, kidney disease, immunosuppression, or females below 18 or above 65 years of age.
Data were collected from electronic medical records (EMRs) retrospectively via chart review for 1 month prior to the intervention. During the preintervention phase, the number of patients treated for an uncomplicated UTI was compared to the number of patients who either returned to the urgent care with unresolved symptoms after initial treatment or were called and needed follow-up for unresolved symptoms post-visit.
Using the current, evidence-based ACOG guidelines for the treatment of uncomplicated UTIs as the foundation, a quality improvement clinical education session was presented to the clinic providers. The intervention advised against the use of C&S laboratory tests in the assessment of uncomplicated UTIs, and showed the evidence supporting this change. With no C&S laboratory tests being ordered for the subject population, postintervention data were collected through chart review for 1 month.
RESULTS
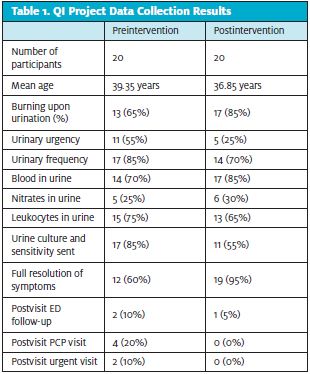
A total of 40 women met the inclusion criteria for both pre- and postintervention sampling. Data were collected from 20 preintervention EMRs and 20 postintervention EMRs. The preintervention data showed the average age of the women in this group to be 39.35 years of age. A C&S was sent for 17 (85%) of the women. When called postvisit, eight (40%) did not have full resolution. Two (10%) stated they needed to follow up in the emergency department. Four (20%) followed up with their primary care provider, and two (10%) returned to an urgent care. (See Table 1). The postintervention data showed the average age of the women in this group to be 36.85 years of age. A C&S was sent for 11 (55%) of the women. When called postvisit, one (5%) did not have full resolution. One (5%) stated they needed to follow up in the emergency department, zero followed up with their PCP, and zero returned to an urgent care. ACOG guideline application resulted in a 30% reduction in the ordering of a C&S in this population with no increase in the rate of follow-up needed in this postintervention group.
CONCLUSIONS
The results of the quality improvement project supported ACOG’s clinical guidelines regarding the assessment of uncomplicated UTIs in the nonpregnant, adult female population. The educational session attended by the providers appeared to play a key role in reducing unnecessary C&S studies and increasing provider awareness of ACOG guidelines for current evidence-based practice. These findings also supported the position that quality patient care can be maintained while healthcare costs are reduced for this population in the urgent care setting.
Projects such as the one discussed here improve patient care outcomes by promoting and implementing evidence-based clinical practice guidelines. Ensuring guideline implementation and sustainability involves ongoing open communication and active involvement by all stakeholders of the urgent care team.
LIMITATIONS
The project improved patient outcomes and reduced unnecessary lab testing, but did have limitations. The sample size was lower than the projected sample size. There was a reduction in the number of patients who presented to the urgent care during the time of data collection, possibly due to the impact of COVID-19. Replication of this project on a larger or continued scale, or using an experimental study format, would be helpful in confirming these findings.
REFERENCES
- Flores-Mireles A, Walker J, Caparon M, Hultgren S. Urinary tract infections: epidemiology, mechanisms of infection and treatment options. Nat Rev Microbiol. 2015;13(5):269-284.
- ACOG.org. Treatment of urinary tract infections in nonpregnant women. 2021. Available at: https://www.acog.org/-/media/project/acog/acogorg/clinical/files/practice-bulletin/articles/2008/03/treatment-of-urinary-tract-infections-in-nonpregnant-women.pdf. Accessed February 3, 2021.
- Poon E, Self L, McLeod S, et al. Uncomplicated urinary tract infections in the emergency department: a review of local practice patterns. CJEM, 2017;20(4):572-577.
- Abou Heidar NF, Degheili JA, Yacoubian AA, Khauli RB. Management of urinary tract infection in women: a practical approach for everyday practice. Urol Ann. 2019;11(4):339-346.
- Mishra B, Srivastava S, Singh K, et al. Symptom-based diagnosis of urinary tract infection in women: are we over-prescribing antibiotics? Int J Clin Pract. 2012;66(5):493-498.
- Uroweb.org. 2021. Available at: https://uroweb.org/wp-content/uploads/EAU-Guidelines-on-Urological-Infections-2018-large-text.pdf. Accessed February, 2021.
- 7. CDC.gov. 2021. Adult treatment recommendations | community | antibiotic Use | CDC. Available at: https://www.cdc.gov/antibiotic-use/community/for-hcp/outpatient-hcp/adult-treatment-rec.html. Accessed February 3, 2021.
- Hopkins L, McCroskey D, Reeves G, Tanabe P. Implementing a urinary tract infection clinical practice guideline in an ambulatory urgent care practice. Nurse Pract. 2014;39(4):50-54.
- Stapleton A. Urine culture in uncomplicated UTI: interpretation and significance. Curr Infect Dis Rep. 2016;18(5):15.
- Salinas M, Flores E, López-Garrigós M, Leiva-Salinas C. 2018. Laboratory test inappropriateness: lessons revisited and clarified in seven questions. J Lab Precis Med. 2018;3:34-47.
- Carroll A. The high costs of unnecessary care. JAMA. 2017;318(18):1748.
Author affiliations: Dianne Treacy Lore DNP, FNP-BC, CPNP-PC, The University of Alabama in Huntsville College of Nursing. Marlena Seibert Primeau DNP, FNP-BC, NHDP-BC, BSHEC, The University of Alabama in Huntsville College of Nursing.