Published on
Resolution
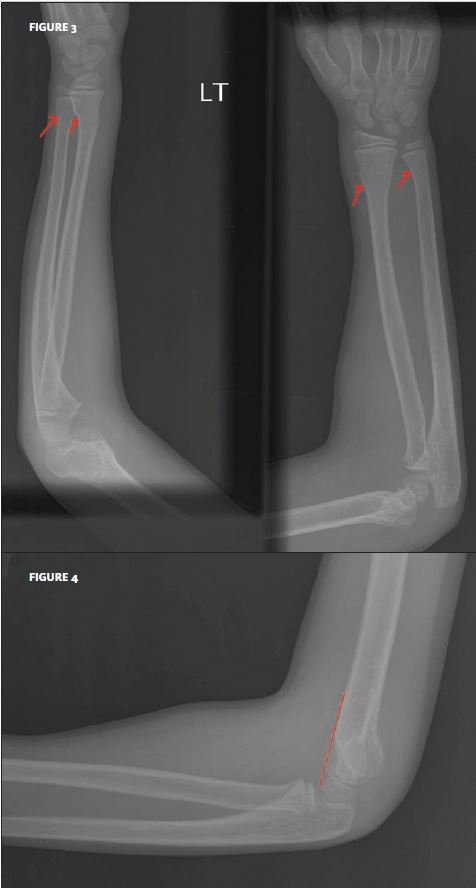
This case offers valuable insight into the phenomenon of pain from one fracture distracting the patient from a second fracture. In this particular situation, the child’s focus was on the wrist pain, yet there were fractures of both the wrist and the supracondylar region.
Drawing a line along the shaft of the humerus (Figure 4) shows that the distal humerus has been rotated backwards. The fact that the distal humerus is in line with the shaft is an indication of a supracondylar fracture. Under normal circumstances, 1/3 of the distal humerus should be in front of this imaginary line.
Also, note the increased anterior fat pad, as well as the posterior fat pad (which is not present under normal circumstances).
The supracondylar fracture is dis- placed, but if the distal pulses are normal and the swelling around the elbow is moderate, then it is legitimate to apply a posterior splint (from the top of the upper arm to the distal fore- arm) and refer for orthopaedic consultation the next day. In this case, the cast must extend to the palm of the patient, in order to immobilize the region of the frac- tures in the wrist.
Acknowledgment: Case presented by Nahum Kovalski, BSc, MDCM.
