Published on
Joshua Russell, MD, MSc, FACEP MD; Ana Echenique, MD, DABR; Steven R. Daugherty, PhD; and Michael Weinstock, MD
Abstract
Background/Objective
A prior study of patients presenting to urgent care (UC) centers with COVID-191 showed that only a small proportion of these ambulatory patients demonstrated significant pathology on chest x-ray (CXR). In this secondary analysis of 636 ambulatory patients with confirmed COVID-19 from greater New York City (NYC), our primary objective was to determine whether the patients’ age and/or gender influenced the likelihood of CXR abnormalities. Secondarily, we aim to describe patterns of specific imaging characteristics and the frequency among each patient gender and age group.
Methods
A database of a large UC company in the greater NYC area was searched for patients with positive SARS-CoV-2 PCR tests who also had a CXR performed at the same UC visit between March 9 and March 24, 2020. Eleven board-certified radiologists, who were informed of the patients’ COVID-19 diagnosis, each reread a subset of CXRs, but were instructed to disregard the initial reading. Their readings were then classified as being either normal, or showing mild, moderate, or severe disease. They subsequently characterized specific findings. Patients were categorized by gender (male or female) and age group (18-40, 41-63, 64-90 years of age). Correlation of severity and characteristics of CXR findings with age and gender was examined using a Pearson Chi-squared test.
Results
Of the 636 CXRs of patients with confirmed COVID-19 reviewed, 363 were from male (57.1%) and 273 were female (42.9%). Patient ages ranged from 18 to 90 years of age, with most (493 patients, or 77.5%) being 30─70 years old. The average age of men and women was not significantly different (51 vs 49 years, respectively). The percentage of patients in each age group and of each gender who demonstrated normal, mild, or moderate-severe abnormalities was not significantly different. Additionally, there were no significant differences in the types of CXR abnormalities, when present, between ages or genders. There was a trend toward multifocal and bilateral disease being more common among women, but this did not reach statistical significance.
Discussion
This is the first study to explore the effects of age and/or gender on CXR findings among patients with COVID-19 in an ambulatory setting. In this subset of patients, neither age nor gender had a statistically significant effect on the severity or type of CXR findings.
INTRODUCTION
The SARS-CoV-2 virus caused the COVID-19 pandemic in early 2020, affecting millions of individuals around the world.2,3 Acute care clinicians have strived to increase their understanding of the disease for purposes of diagnosis, prognosis, and management of afflicted patients as well as to mitigate the extent of disease spread.
Age and gender have been shown to influence the likelihood of developing severe illness and mortality in some series of patients with COVID-19. Multiple series of hospitalized Chinese patients have demonstrated a linear increase in the risk of death with increasing age.4,5 While several studies have failed to demonstrate a relationship between gender and risk of death, Shi, et al did find a significantly higher risk of severe disease among men in a group of 487 hospitalized patients in central China.6 However, the role of age and gender, as it pertains to radiographic disease severity, has not been examined among ambulatory patients.
Disease severity differs between ambulatory patients and those requiring hospitalization. Imaging among hospitalized patients tends to demonstrate abnormalities with much higher frequency than among outpatients (84% vs 42%).1,7 Overall, the imaging changes tend to progress through the illness and peak on days 10─12.3,8
While many early observational studies have focused on the value of chest computed tomography (CT) in diagnosing COVID-19 pneumonia,3,9-11 this imaging modality is rarely available in UC centers. Plain film radiography of the chest is an established, safe, cost-effective, and nearly ubiquitous imaging modality in urgent care centers. Because the vast majority of patients with COVID-19 present with mild respiratory symptoms, evaluations are much more likely to take place in ambulatory settings, such as UC centers.2 However, to date, most studies have examined the role of CXR in the evaluation of hospitalized patients with COVID-19.
In the only other study to date examining the relationship between age, gender, and severity of CXR findings in patients with COVID-19, Borghesi, et al reviewed CXRs of 783 hospitalized Italian patients with confirmed COVID-19 and found that the severity of CXR abnormalities was positively correlated with increasing age.12 They also found that men had a higher likelihood of severe abnormalities than women, but only among individuals aged 50─79 years of age. No prior studies have examined whether specific patterns of CXR findings are correlated with age or gender.
The aim of this study was to determine if there were differences in CXR findings in ambulatory patients based on age (primary endpoint) or gender (secondary endpoint).
METHODS
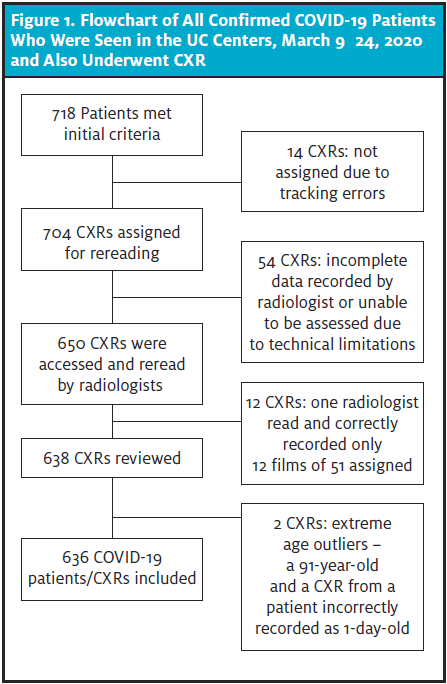
The electronic medical record (EMR) database of a large UC network in greater New York City (NYC) and New Jersey (NJ) was queried, identifying 718 patients with positive SARS-CoV-2 PCR testing who also had a CXR during a UC visit between March 9 and March 24, 2020 (during the time that greater NYC was the epicenter for COVID-19). These patients’ CXRs were initially divided among 14 board-certified radiologists. However, due to technical issues, only 12 radiologists were able to participate in the study. These individuals were assigned approximately 50 CXRs each, except for two of the radiologists who reviewed an additional 50 CXRs to compensate for the two radiologists who were unable to participate.
Most participants read 47 to 100 films. One radiologist, however, read only 12 films. These readings were excluded from this study because the number of cases was far below the contributions of the other participants. This resulted in a total analyzed sample of 636 CXRs (Figure 1).
The participating radiologists were given oral and written instructions to first categorize films as normal, mild, moderate, or severe disease. For those classified as abnormal, they were asked to describe the specific findings. The initial CXR readings were part of these patients’ medical records, but the radiologists were instructed to disregard the initial reports when rereading the films. Participating radiologists were informed prior to rereading that the CXRs were from patients with confirmed COVID-19.
Statistical analysis
All statistical analyses were conducted using the statistical program PSPP. The Pearson two-tailed chi-squared test was used to analyze categorical tables and a two-tailed t-test was used to analyze the combination of categorical and interval data. Findings for which there were no CXRs with the finding among certain groups (eg, young patients with pleural effusions) were excluded from the chi-squared analysis because empty cells render interpretation problematic.
Patients were divided into three general groups based on phases of adulthood: young adult (18─40 years), middle-aged (41─63 years), and elderly (64─90 years). CXR reads were also divided into three categories: normal, mildly abnormal, and moderately/severely abnormal. Because there were relatively few severely abnormal CXRs, the moderate and severe categories were combined to improve the robustness of our statistical analyses. Practically speaking, the distinction between moderate and severe CXR abnormalities is also of less clinical significance than the distinction between normal and mild, for example.
RESULTS
Of the 636 CXRs reviewed among patients with confirmed COVID-19, 363 were male (57.1%) and 273 were female (42.9%). Patient ages ranged from 18 to 90 years of age, with most (493 patients, or 77.5%) being 30─70 years old (Table 1 and Figure 2). The average age of the women (49 years) in this sample was 2 years younger than the average age of the men (51 years), although this difference was not statistically significant. (t= 1.65, p=.10).
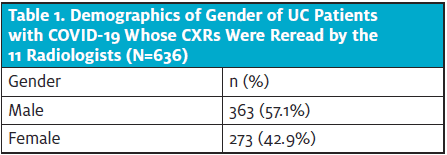
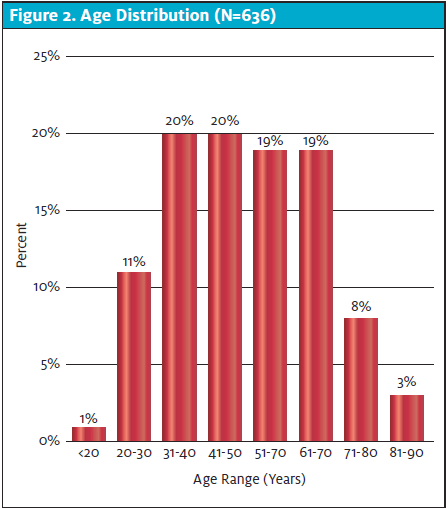
Table 2 summarizes the overall findings of radiologists when rereading the CXRs. Notably, among the 636 CXRs included, 58.3% were read as normal. Among the abnormal cases (41.7%), 195 were classified as mild disease, 65 were classified as moderate disease, and five were classified as severe disease. Interstitial changes and ground glass opacities (GGO) were the predominant descriptive findings in 151 (23.7%) and 120 (18.9%) of the total, respectively. Location of the abnormalities was in the lower lobe in 215 (33.8%), bilateral in 133 (20.9%), and multifocal in 154 (24.2%). Effusions and lymphadenopathy were uncommon.
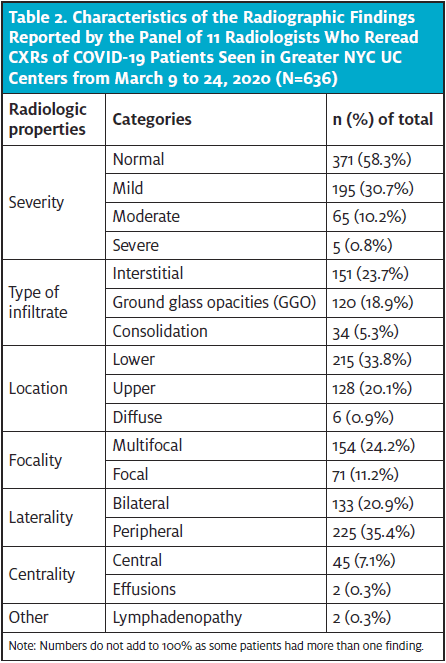
Note: Numbers do not add to 100% as some patients had more than one finding.
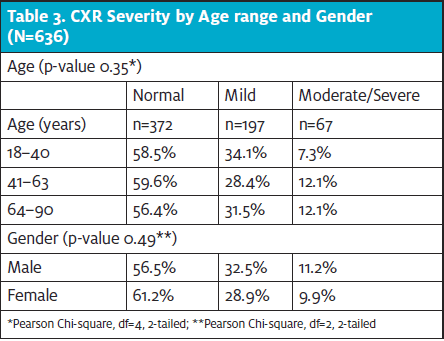
When examining for associations of abnormalities with age and gender, neither showed a statistically significant relationship with the classification of CXR severity (Table 3). In other words, the likelihood of normal, mild, moderate/severe abnormalities was the same across age groups and genders.
With patients having abnormal CXR findings (mild or moderate/severe), there were no statistically significant differences based on gender. Although women were more likely to have multifocal and bilateral abnormalities, this difference fell short of the usual level of statistical significance (ie, p<0.05). None of the other types of abnormalities showed any differences related to gender. (See Table 3.)
With patients having abnormal CXR findings (mild or moderate/severe), there were no statistically significant differences based on patient’s age. Similarly, no specific patterns of radiographic abnormalities were correlated with age.
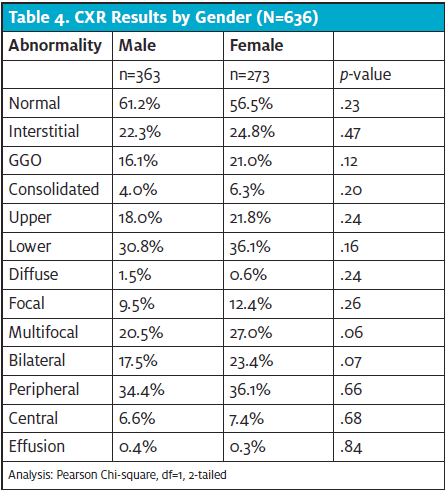
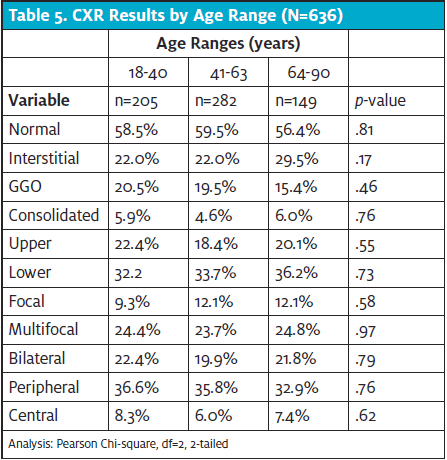
Figure 3. Multifocal mixed central and peripheral linear infiltrates extending out to lung periphery with superimposed, ill-defined patchy opacities at the bilateral lung bases. Lung apices spared. Overall low volume, study concerning for hypoventilation.
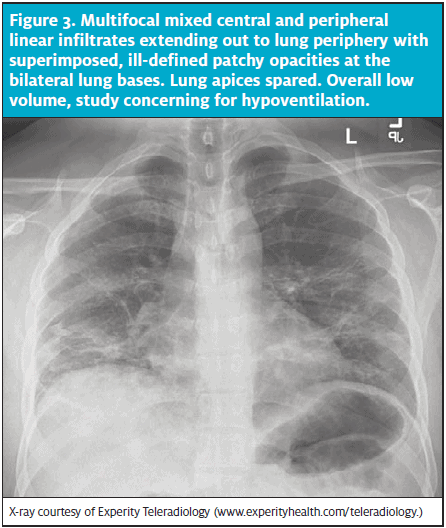
X-ray courtesy of Experity Teleradiology (www.experityhealth.com/teleradiology.)
LIMITATIONS
Studies of this type are inherently limited due to their retrospective and observational nature. Only a single CXR series was obtained for each patient. Because patients presented at various phases of illness, it is impossible to know how their CXR appearance may have progressed through their clinical course. Additionally, the patients’ underlying health histories and baseline CXRs were not available and therefore, it is unclear whether abnormalities identified may be related to chronic conditions.
Regarding CXR interpretation, although the radiologists were instructed not to let the initial CXR read or knowledge of COVID-19 diagnosis influence their interpretation, they were not blinded to this information. Therefore, this knowledge might have impacted their CXR classifications. We also did not perform an assessment of inter-rater reliability between radiologists on the rereads. The difference in percentage of normal classification across participants, however, suggests that individual differences among radiologists do exist.
The initial CXRs were obtained at the discretion of the treating provider. It is likely that variations in the clinical approaches and CXR utilization among providers affected which patients had CXRs obtained and, therefore, available for analysis among those with COVID-19. The direction of any associated bias is difficult to predict because many diverse factors influence providers’ decisions about imaging patients with respiratory complaints.
DISCUSSION
This report is a secondary analysis examining the effects of gender and age on a large cohort of COVID-19 patients presenting to a group of greater NYC UC centers. In this large group of ambulatory patients with confirmed COVID-19, neither age nor gender affected the CXR findings in a significant way. Only one other study to date has examined the effects of age or gender on radiographic abnormalities in patients COVID-19. Interestingly, Borghesi, et al did find significant differences in the CXR findings among hospitalized men and women of different ages with COVID-19, with the likelihood of CXR abnormalities being higher in older patients and men.12
Apart from differences between hospitalized and ambulatory patients, the discrepancy in findings between these studies is also likely largely attributable to the differences in disease severity between the population in each study. In the Borghesi, et al study, multiple CXRs were reviewed for each patient and only the most severely abnormal CXR was included.12 Whereas, in our study, only a single CXR was reviewed from each patient when they presented to an outpatient setting. It is probable that some of these UC patients developed more severe radiographic findings later in the course of their illness.
Additionally, patients in this study were community-dwelling; the older patients likely had a disproportionately high functional status compared with average individuals of the same age. For example, an 85-year-old who is presenting to an ambulatory care setting is generally healthier than an average patient of the same age, whereas a 45-year-old patient presenting to UC is more likely to be of average health for their age. This phenomenon would tend to dilute or negate effects of age due to a skewing of the sample coming from the healthier tail of the distribution for any age especially among older patients.
Regardless of whether or not age or gender has any effect on CXR appearance at later or more severe stages of illness, the data from our sample indicate that age and gender do not seem to affect the likelihood or variety of CXR abnormalities seen at the time of UC presentation. This finding is of value to the UC clinician because it suggests that neither age nor gender should strongly influence the decision to obtain a CXR with confirmed or suspected COVID-19.
CONCLUSION
In this large group of ambulatory UC patients with confirmed COVID-19, neither age nor gender significantly affected the likelihood of more severe CXR abnormalities, nor the specific types of abnormalities.
(This study was IRB-approved and granted waiver of consent and full waiver of HIPAA authorization. No funding was obtained for this study.)
Citation: Russell J, Echenique A, Daugherty S, Weinstock M. Chest x-ray findings among urgent care patients with COVID-19 are not affected by patient age or gender: a retrospective cohort study of 636 ambulatory patients. J Urgent Care Med. July-August 2020. Available at? https://www.jucm.com/chest-x-ray-findings-among-urgent-care-patients-with-covid-19-are-not-affected-by-patient-age-or-gender-a-retrospective-cohort-study-of-636-ambulatory-patients/.
References
- Weinstock MB, Echenique A, Russell JW, et al. Chest x-ray findings in 636 ambulatory patients with COVID-19 presenting to an urgent care center: a normal chest x-ray is no guarantee. J Urgent Care Med. 2020;14(7):13-18.
- Guan WJ, Ni ZY, Hu Y, et al. Clinical characteristics of coronavirus disease 2019 in China. New Engl J Med. February 28, 2020. [Epub ahead of print]
- Shi H, Han X, Jiang N, et al. Radiological findings from 81 patients with COVID-19 pneumonia in Wuhan, China: a descriptive study. Lancet Infect Dis. 2020;20(4):425-434.
- Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395(10229):1054–1062.
- Wang Z, Yang B, Li Q, et al. Clinical features of 69 cases with coronavirus disease 2019 in Wuhan, China. Clin Infect Dis. 2020;
- Shi Y, Yu X, Zhao H, et al. Host susceptibility to severe COVID-19 and establishment of a host risk score: findings of 487 cases outside Wuhan. Crit Care. 2020;24(1):108.
- Lomoro P, Verde F, Zerboni F, et al. COVID-19 pneumonia manifestations at the admission on chest ultrasound, radiographs, and CT: single-center study and comprehensive radiologic literature review. Eur J Radiol Open. April 4, 2020. [Epub ahead of print]
- Wong HYF, Lam HYS, Fong AH-T, et al. Frequency and distribution of chest radiographic findings in COVID-19 positive patients. Radiology. March 27, 2019. [Epub ahead of print]
- Xu X, Chengcheng Y, Jing Q, et al. Imaging and clinical features of patients with 2019 novel coronavirus SARS-CoV-2. Eur J Nucl Med Mol Imaging. 2020;47:1275–1280.
- Ng MY, Lee EYP, Yang J, et al. Imaging profile of the COVID-19 infection: radiologic findings and literature review. Radiol: Cardiothor Imag. doi.org/10.1148/ryct.2020200034.
- Bernheim A, Mei X, Huang M, et al. ChestCTfindings in coronavirus disease-19 (COVID-19): relationship to duration of infection. Radiology. February 20, 2020. [Epub ahead of print]
- Borghesi A, Zigliani A, Masciullo R, et al. Radiographic severity index in COVID-19 pneumonia: relationship to age and sex in 783 Italian patients. Radiol Med. May 1, 2020. [Epub ahead of print]

Joshua Russell, MD, MSc, ELS, FACEP, FCUCM

Ana Echenique, MD

Michael B. Weinstock, MD
