Published on
Urgent message: Syncope in pediatric patients may be attributed to a wide variety of sources. As such, it is essential to keep a broad differential and to eliminate potentially life-threatening etiologies.
Nehal Bhandari, MD, FAAP and Abbas Zaidi, MD, FAAP
CASE PRESENTATION
A 12-year-old previously healthy female presents to urgent care with several episodes of “blacking out” over the past 4 days. Each episode has occurred when she stands up from a sitting or supine position and lasts a few seconds. She reports feeling dizzy when this happens. The episodes do not appear to be related to exercise. She states that she has only had one bottle of water in the last 24 hours. She has also had intermittent frontal headaches for the last 4 days and left sided tinnitus for the last 3-4 months. Earlier this week, she was diagnosed with vasovagal syncope and instructed to increase fluid and electrolyte intake and to follow up with her primary care physician. With a repeat episode, mom brought her to urgent care for further evaluation.
She denies chest pain, palpitations, difficulty breathing, phonophobia, or photophobia. No head injury.
Vital Signs
- BP 120/78
- HR 53
- Temp 36.8⁰C
- RR 18
- O2 100%
Physical Exam
The patient is overall well-appearing, sitting up in the exam bed on her phone.
Cardiac Exam
Regular rate and rhythm without murmurs, rubs, or gallops, 2+ radial and femoral pulses, cap refill <2 seconds.
Abdomen
Soft, nontender, no hepatosplenomegaly.
Neuro
She is alert and oriented x 4, pupils are equal, round, and reactive to light, cranial nerves 2─12 are intact, full strength in all four extremities. Gait not examined per patient’s request as she was worried about precipitating a syncopal episode. The remainder of her exam is grossly normal.
OVERVIEW
Syncope is an abrupt, transient loss of consciousness due to decreased blood pressure and cerebral blood flow. It is a common presenting complaint in pediatric emergency departments (ED) that accounts for as many as 3% of all ED visits in children.1 Girls are impacted more often than boys.2 As many as 30% to 50% of children will have had at least one syncopal episode by the time they reach 18 years of age.3
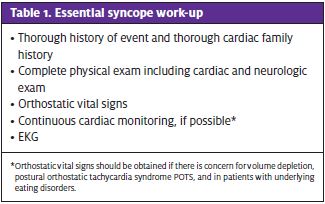
The etiology of syncope varies by age and may be due to circulatory, cardiac, metabolic, neurologic, situational, or even psychiatric processes. While syncope in pediatric patients is most commonly benign, especially in an adolescents, an organized approach is necessary in order to avoid missing serious and life-threatening etiologies (Table 1).
DIFFERENTIAL DIAGNOSIS
Cardiac
Cardiac etiologies of syncope may be life-threatening and require prompt recognition of the underlying cardiac disorder and subsequent disease-specific management. The differential for cardiogenic syncope can be divided into two main categories: arrythmias and structural abnormalities.
Arrythmias include Brugada syndrome, prolonged QT syndrome, AV block, Wolff-Parkinson-White, catecholaminergic polymorphic ventricular tachycardia (CPVT), etc.
Structural abnormalities include hypertrophic cardiomyopathy, left-sided obstructive lesions including aortic stenosis, pulmonic stenosis, dilated cardiomyopathy, etc.1
The history features that most suggest a possible underlying cardiac etiology include palpitations, syncope occurrence with exercise, and a family history of sudden death or cardiomyopathy. Syncope that is induced by exercise is particularly worrisome and mandates urgent referral and investigation.4-6
Peak exercise increases catecholamine release and cardiac work creating the substrate for potential lethal arrythmias. By contrast, the period immediately following exertion is associated with vasodilation and shifting autonomic states, making noncardiogenic syncope more likely. The timing of a syncopal event (during vs postexercise) is an important distinguishing factor. It is also important to discern if palpitations or chest pain were present before the episode.7
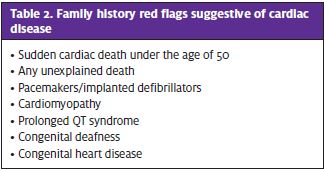
Asking a detailed family history helps to discern life-threatening arrythmias that are caused by genetic conditions (Table 2). It is important to ask about a history of sudden cardiac death in a relative 50 years or younger or any unexplained deaths, drowning, or fatal motor vehicle accidents. Further cardiac questioning should include whether there is a family history of pacemakers/implanted defibrillators, cardiomyopathy, prolonged QT syndrome (or congenital deafness which can be associated with prolonged QT), or congenital heart disease.1
Neurologic
Syncope must be differentiated from an event that was precipitated by a seizure. Myoclonic extremity movements that occur at the same time as syncope suggest an underlying seizure disorder. However, one should note that anytime there is cerebral hypoperfusion, convulsive movements are possible. This is known as convulsive syncope. This is different from epilepsy as the myoclonic movements occur after loss of consciousness and tonus instead of at the same time as syncope. This may be difficult to discern on the basis of history alone.4
Seizures are more likely to occur in the supine position compared with vasovagal syncope. Jaw locking is also more common. It is essential to determine if there was a postictal period, loss of bowel or bladder control, or tongue biting, as these features make seizures more likely. 4
Persistent neurologic deficits or failure to return to neurologic baseline are red flags that indicate etiology more serious than benign syncope. A thorough neurologic exam must be done for all patients presenting with syncope. Any focal neurologic findings on exam should prompt immediate neuro-imaging and/or neurology consultation.
Postural Orthostatic Tachycardia Syndrome
POTS is a type of autonomic dysfunction in which patients are intolerant to positional changes which lead to development of excessive tachycardia. A subset of patients will present with constellation of symptoms that are associated with lightheadedness, dizziness, palpitations, and sometimes syncope. The diagnostic criteria for POTS is evolving, but it is an increase in heart rate of 30 beats per minute or more or over 120 bpm within the first 10 minutes of standing, in the absence of orthostatic hypotension, is generally considered diagnostic. It is important to also get a detailed review of systems as POTS can involve multiple organ systems and can have a constellation of symptoms.8-12
Neurocardiogenic (Vasovagal)
The most common cause of pediatric syncope is vasovagal (also known as autonomic, neurocardiogenic, or reflex) syncope.3 It accounts for nearly 80% of cases of pediatric syncope.2 Patients may have a prodrome followed by a syncopal episode that lasts 1 minute or less. Prodrome features may include dizziness, feeling overheated, nausea, or changes in vision. Vasovagal syncopal episodes are often followed by a stressor such as emotional distress or prolonged standing.13 Therefore, it is important for the patient and witnesses to describe the episode in detail as well as the position of the patient prior to the syncopal episode. This type of syncope does not typically occur while supine.4 It is also important to find out whether the patient had anything to eat or drink that day as reflex syncope is often triggered by dehydration and fasting.
Situational syncope, which falls under the category of vasovagal syncope, can occur after micturition, defecation, hair grooming, sneezing, or coughing.2
Psychogenic
Psychogenic syncope frequently occurs in times of stress or high emotion and is unlikely to occur in children under 10 years of age. These psychogenic episodes may be a manifestation of underlying conversion disorder.1 Self-resolving syncope that lasts longer than 10 minutes is unlikely physiologic and likely suggests a potential psychological etiology.4
Other (Hematologic, Metabolic, Drug Use, Pregnancy)
While these conditions are uncommon in pediatrics, any situation resulting in blood loss, fluid shifting, or severe electrolyte abnormalities can contribute to neurocardiogenic, neurologic, or cardiac syncope.
Anemia may be present in menstruating adolescents. It is important to ask adolescent female patients about their last menstrual periods and the number of daily pads used to evaluate for excessive blood loss. Gastrointestinal blood loss is uncommon in children, but any patient with abdominal discomfort should be asked about stool color to screen for a possible upper or lower GI source.
The likelihood of a metabolic cause in an otherwise healthy child is low, but any patient who has renal insufficiency or other metabolic chronic disease may be more likely to have a syncopal episode because of a fluid-electrolyte imbalance.
Lastly, drug use and pregnancy are important potential causes in adolescent patients.
HISTORY AND EXAM PEARLS
Most patients are asymptomatic by the time they are evaluated, and most will have a normal physical exam. It is unlikely that another syncopal episode will occur during evaluation. Therefore, a detailed history of the syncopal event as well as thorough past medical history and family history are essential.4 The history should provide clues to discern possible neurologic, cardiac, or neurocardiogenic causes. It is important to ask about cardiac symptoms, if the episode occurred during exercise, if there was a prodrome before the event, if there was any extremity jerking, and how long it took the patient to return to neurologic baseline.
VITAL SIGNS
Orthostatic vitals (supine, sitting, and standing) should be obtained if there is concern for volume depletion or if the patient has an underlying eating disorder. A patient is considered to have orthostasis if there are any of the following: increase in pulse by >10 beats per minute, decrease in systolic blood pressure by >20 mmHG, or decrease in diastolic blood pressure by >10 mmHG. This indicates hypovolemia and a potential fluid deficit of 10 to 15 mL/kg. However, positive orthostatic vitals do not rule out other causes of syncope. When possible, it is recommended that patients stay on continuous cardiac monitoring to evaluate heart rate and rhythm.2
A straightforward supine or seated cardiac examination can be insufficient to elicit a murmur from a previously undiagnosed myopathy or the dynamic physiology associated with postural orthostatic tachycardia syndrome. Therefore, the physical examination should include a dynamic auscultation, vital signs, and evaluation of other exam features such as signs of connective tissue disease and neurological abnormalities. It is important to include assessment of capillary refill, pulses in upper and lower extremities, and evaluation for lower extremity edema as well as hepatomegaly. Muffled heart sounds and a friction rub are characteristic of acute pericarditis. A systolic ejection murmur that increases in intensity with standing or with Valsalva is suggestive of hypertrophic cardiomyopathy.2
DIAGNOSTICS
EKG
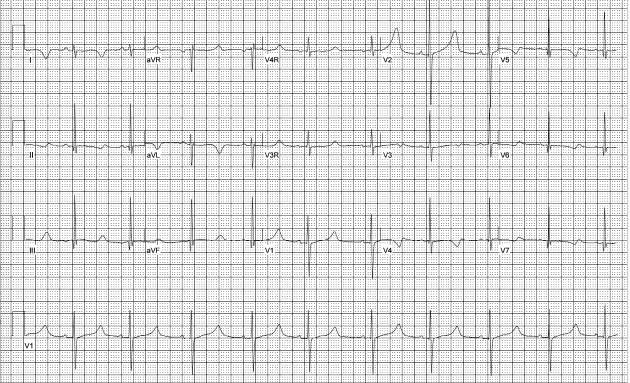
Electrocardiography is an important tool in the evaluation of syncope to determine if a potential cardiac etiology is present. This is a routine component of the syncope evaluation even when no residual symptoms or exam abnormalities are present. Abnormalities on EKG may fully explain the episodes or indicate the need for additional testing. It is important to note that when combined with a noncontributory history and examination, a normal EKG is very effective at excluding cardiac etiologies.
The QT interval, which varies with heart rate, must be measured closely. The Bazett formula (QTc = (QT)/(ÖRR) is commonly used.2 The upper limit of a corrected QT interval (QTc) is generally 450 milliseconds.2 QTc values of 470 milliseconds or longer are especially concerning for prolonged QT syndrome (Figure 1). In patients with prolonged QT syndrome, syncope is often related to torsades de pointes and death is due to ventricular fibrillation.2
ST elevation in V1 and V2 may be suggestive of Brugada syndrome. Large amplitude QRS waves with LVH and narrow Q waves are often seen in hypertrophic cardiomyopathy.2 Wolff-Parkinson-White syndrome is characterized by a preexcitation delta wave as well as conduction abnormalities such as AV block and ventricular hypertrophy.1
Additional cardiac testing which may be considered in conjunction with cardiology consultation includes echocardiogram, exercise stress testing, and ambulatory ECG monitoring (eg, Holter or event monitoring).
Laboratory Evaluation
Serum labs are rarely necessary in the work-up of syncope in previously healthy pediatric patients. While hypoglycemia is a potential etiology for syncope, serum glucose levels are often normal by the time a patient is evaluated.
Adolescent patients, however, are a special population that may require more testing than younger children. All adolescent females should be screened for pregnancy.1 Serum or urine drug screens can be considered if there is clinical suspicion for drug use. Common disorders such as anemia and moderate iron deficiency, particularly in adolescent females with menstrual cycle irregularities, can be easily screened with a set of complete blood count and iron studies. Other considerations include thyroid disorders which should be based on clinical suspicion. Stable patients can also be referred to their primary care providers for thyroid and iron studies if these are not easily obtainable in the urgent care setting.
For patients with underlying chronic medical problems (type I diabetes mellitus, anorexia, renal insufficiency, etc.), it may be helpful to obtain screening labs that include a metabolic panel and urinalysis.
Other diagnostics
Other diagnostic testing that may be helpful when coordinated through outpatient follow-up includes stress testing, tilt table, electroencephalography, etc. There is no role for chest radiography in the acute setting unless otherwise indicated.
MANAGEMENT AND FOLLOW-UP
ED referral is necessary for patients who have focal neurologic or cardiac findings, significant metabolic abnormalities, multiple red flags, or a neurologic exam that fails to return to baseline.
Outpatient cardiology follow-up is recommended for patients who have mild EKG abnormalities, family history red flags (Table 2), or if the syncopal episode occurred with exercise. These patients should not participate in sports until cleared by cardiology.
Outpatient neurology follow-up is recommended if there is concern for possible seizure-like activity in a patient who has returned to baseline and has a normal neurologic exam.
Patients with single isolated episodes of syncope that are likely due to a neurocardiogenic etiology do not require extensive work-up or subspecialty referral. These patients should be instructed to lie supine with their lower extremities elevated in order to increase blood flow to the heart if they ever feel symptoms of pre-syncope again. Reflex syncope can be treated by hydration and increasing salt intake. Exercise may also be beneficial. Diuretics such as alcohol and caffeine should be avoided to prevent dehydration. These patients should be instructed to follow up with their primary care physician after discharge from the ED or urgent care.
CASE CONCLUSION
The patient’s syncope was presumed pathologic because of associated headache, tinnitus, bradycardia, and multiple syncopal episodes. The patient was referred to the ED where a head CT showed hydrocephalus and a subsequent MRI revealed a ganglioglioma obstructing her ventricular drainage. She was admitted for surgery and initiation of chemotherapy.
References
- Cannon B, Wackel P. Syncope. Pediatr Rev. 2016;37(4):159-168.
- Welch-Horan TB, Shenoi RP. Syncope. In: Shaw KN, Bachur RG, eds. Fleisher & Ludwig’s Textbook of Pediatric Emergency Medicine. 7th ed. Wolters Kluwer; 2016:912-922.
- Dalal AS, Hare GFV. Syncope. In: Kliegman RM, Geme JWS, Blum NJ, Shah SS, Tasker RC, Wilson KM, eds. Nelson Textbook of Pediatrics. 21sted. Elsevier; 2020:566-571.
- Ikiz MA, Cetin II, Ekici F, et al. Pediatric syncope: Is detailed medical history the key point for differential diagnosis? Pediatr Emerg Care. 2014;30(5):331-334.
- Calkins H, Seifert M, Morady F. Clinical presentation and long-term follow-up of athletes with exercise-induced vasodepressor syncope. Am Heart J. 1995;129(6):1159-1164.
- Sakaguchi S, Shultz JJ, Remole SC, et al. Syncope assoociated with exercise, a manifestation of neurally mediated syncope. Am J Cardiol. 1995;75:476-481.
- Schunk PC, Ruttan T. Pediatric syncope: high-risk conditions and reasonable approach. Emerg Med Clin North Am. 2018;36(2):305-321.
- Grubb BP. Postural tachycardia syndrome. Circulation. 2008;117:2814-2817.
- National Institute of Health NIoNDaS. Postural Tachycardia Syndrome Information Page. Available at: https://www.ninds.nih.gov/Disorders/All-Disorders/Postural-Tachycardia-Syndrome-Information-Page. Accessed July 25, 2021.
- Raj SR. The Postural tachycardia syndrome (POTS): pathophysiology, diagnosis & management. Indian Pacing and Electrophysiology Journal. 2006;6(2):84-99.
- Freeman R, Wieling W, Axelrod FB, et al. Consensus statement on the definition of orthostatic hypotension, neurally mediated syncope and the postural tachycardia syndrome. Auton Neurosci. 2011;161(1-2).
- Singer W, Sletten DM, Opfer-Gehrking TL, Brands CK, Fischer PR, Low PA. Postural Tachycardia in Children and Adolescents: What is Abnormal? The Journal of Pediatrics. 2012;160(2):222-226.
- Zavala R, Metais B, Tuckfield L, et al. Pediatric syncope: a systematic review. [Epub ahead of print]. Pediatr EmergeCare. 2020;00(00):1-4.
Author affiliation: Nehal Bhandari, MD, FAAP, Emory University School of Medicine. Abbas Zaidi, MD, FAAP, Emory University School of Medicine.