Published on
Differential Diagnosis
- Second-degree heart block
- Third-degree heart block
- Junctional rhythm
- Q waves in the inferior leads, indicative of previous MI or LBBB
- Acute inferior MI
Diagnosis
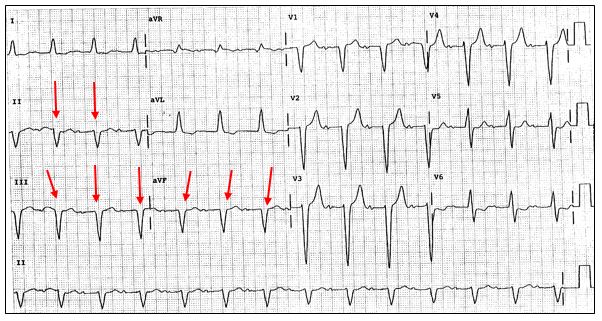
This ECG shows a sinus rhythm (a P wave preceding each QRS) with a rate of 80, but the PR interval is prolonged, reflecting first-degree AV block (normal PR interval is 120-200 ms).
As there is a p wave before each QRS, this is not a junctional rhythm.
Second-degree block involves a dropped beat (either Mobitz 1 or 2). Third-degree AV block has complete absence of AV conduction without relation of the p waves and the QRS complexes, typically at a rate in the 30s. Neither second- or third-degree AV block is reflected on this ECG.
There is no evidence of ST elevation in the inferior leads (II, III, aVF), so this is not an acute inferior MI.
The Q waves present in the inferior leads are likely indicative of a previous MI. Note that with the widened QRS complex (normal is 80-120 ms) there is a nonspecific intraventricular conduction delay which could also indicate that left bundle branch block (LBBB) is present and the Q waves present inferiorly could also be due to the LBBB.
Learnings/What to Look for:
- The inferior leads, II, III, and aVF are limb leads which reflect changes at the bottom portion of the heart, typically with blood supply from the right coronary artery (RCA)
- Q waves are present if there is a Q-wave which is one box (0.04 ms) wide and one box deep
- In addition to evaluating ECGs for acute ischemia, they should be checked for possible past infarction
Pearls for Urgent Care Management and Considerations for Transfer
- Evidence of old MI can be incidentally found on ECGs
- Assess for ongoing ischemia clinically (chest pain/discomfort, shortness of breath, diaphoresis, arm/shoulder/neck/jaw pain) and with assessment of the ECG for ST elevation, ST depression, or T wave inversion
- If the patient is asymptomatic and the Q waves are found incidentally, further evaluation can be done as an outpatient
- If there are clinical or ECG changes of ischemia, the patient should be emergently transferred to the ED