
Published on
Urgent message: This article will guide you through the differential diagnosis, management and disposition of pediatric patients presenting with acute abdominal pain.
KAYLEENE E. PAGÁN CORREA, MD, FAAP
Introduction
“My tummy hurts.” That is a simple statement that shows a common complaint from children who seek care in an urgent care or emergency department.1 But the diagnosis in such patients can be challenging for a clinician because of the diverse etiologies. Acute abdominal pain is commonly caused by self-limiting conditions but also may herald serious medical or surgical emergencies, such as appendicitis. Making a timely diagnosis is important to reduce the rate of complications but it can be challenging, particularly in infants and young children. Excellent history-taking skills accompanied by a careful, thorough physical exam are key to making the diagnosis or at least making a reasonable conclusion about a patient’s care.2
This article discusses the differential diagnosis for acute abdominal pain in children and offers guidance for initial evaluation and management of pediatric patients presenting with this complaint.
Pathophysiology
Abdominal pain localization is confounded by the nature of the pain receptors involved and may be classified as visceral, somatoparietal, or referred pain. Visceral pain is not well localized because the afferent nerves have fewer endings in the gut, are not myelinated, and are bilateral, entering the spinal cord at several levels. Children perceive visceral pain generally over the epigastric, periumbilical or suprapubic region.
Contrary to visceral pain, somatoparietal pain is well localized, intense (sharp), and associated with one side or the other because the nerves associated are numerous, myelinated and transmit to a specific dorsal root ganglia. Somatoparietal pain receptors are principally located in the parietal peritoneum, muscle and skin and usually respond to stretching, tearing or inflammation. Referred pain is generally well localized but distant from the affected site. It arises when visceral pain fibers affect the somatic nerve fibers in the spinal cord.
History, Symptoms and Laboratory Diagnosis
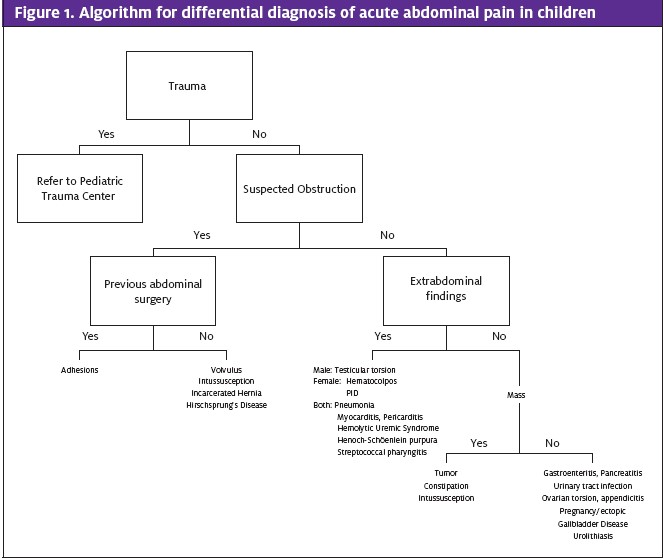
Often, history is the most important component in making the diagnosis. The age and sex of a patient, the order of onset of symptoms, progression and quality of pain, associated symptoms (fever, vomiting, diarrhea, constipation, anorexia, rash, altered mental status, dysuria, hematuria or vaginal secretions), gynecologic and surgical history and history of recent trauma are important to narrow the differential diagnosis in addition to the physical exam (Figure 1). Some of the indicators on the history and physical exam that should prompt surgical evaluation include: bilious vomiting, pain worseing with movement, involuntary guarding, rebound tenderness and tenderness with percussion or history of abdominal trauma. Patients with findings concerning for obstruction, peritoneal irritation, incarcerated hernia, systemic life-threatening conditions (diabetic ketoacidosis and hemolytic uremic syndrome), tubo- ovarian abscess or ruptured ectopic pregnancy should be transferred for further management.3
Children with abdominal pain who are well-appearing, otherwise healthy, have a normal physical exam and tolerate feedings may not require laboratory or imaging studies and can be discharged home with close follow up by primary physician within 24 hours unless intussusception is suspected. Ancillary studies should be performed when history or physical examination suggests a concerning diagnosis. The choice of test should be based on the diagnoses being considered and a patient’s age. Initial work up may include a complete blood count (CBC), basic metabolic panel, sedimentation rate, c-reactive protein (CRP) level, and urinalysis, although other specific laboratory studies such as lipase, amylase, liver enzymes, testing for pregnancy, gonorrhea and chlamydia, and wet prep may be appropriate, depending upon the conditions being considered. Laboratory studies are usually not diagnostic but can be used to confirm a clinician’s suspicion. Analgesia should be provided according to a patient’s reported pain. Although in the past administration of morphine to children with acute abdominal pain for pain reduction was believed to affect the examination, several studies have concluded otherwise.4,5 Imaging studies can be used to confirm the suspected diagnosis. If further imaging or repeated abdominal exams are necessary to clarify the diagnosis, a patient may have to be transferred to a hospital that has a pediatric surgery service. Abdominal films may demonstrate obstruction (air fluid levels, distended bowel, or sentinel bowel loops), perforation (free air), fecalith, or constipation.6 Chest radiograph can be used if there is a concern for basilar pneumonia or signs of myocarditis. For children with suspected midgut volvulus, achalasia, or duodenal web, an upper gastrointestion- al (GI) series with contrast is the best examination. Ultra- sound is noninvasive, relatively inexpensive and does not use ionizing radiation, but accuracy varies depending on the ultrasonographer’s technique. Imaging may show pyloric stenosis, intussusception (doughnut sign), appen- dicitis (noncompressible, aperistaltic tubular structure arising from the cecum with periappendicial fluid and walls > 6 mm in diameter), ovarian torsion, ectopic pregnan- cy, cholelithiasis and urolithiasis. Computed tomography (CT) scan is helpful for identifying nephrolithiasis, appendicitis, pancreatitis, abdominal masses, inflammatory bowel lessions, and intra-abdominal abscesses but it can be invasive, may require intravenous (IV), oral, or
Causes of Acute Abdominal Pain Related to Obstruction
Volvulus
Improper rotation and fixation of duodenum and colon (malrotation) makes the midgut vulnerable to volvulus. The volvulus twists about the superior mesenteric artery axis, causing the midgut to lose its blood supply, leading to development of ischemic necrosis. Most patients with volvulus present during the first year of life, and particularly the first month of life. The condition manifests as bilious vomiting, abdominal distension, GI bleeding, and subsequent shock.7 A patient with volvulus should be resusci- tated (ABCs), receive noth- ing per os (NPO), have a nasogastric (NG) tube placed for decompression, be started on broad-spectrum antibiotics to cover the GI tract and should be transferred for further imaging and surgical evaluation.8 Expeditious management may make the difference between a condition that is completely reversible and one that results in loss of a large segment of intestine. An upper GI series is the study of choice, and laparotomy is required for definitive treatment.
Intussusception
Intussusception is the telescoping of one portion of the bowel into its distal segment; most commonly the terminal ileum invaginates into the cecum. It is one of the most frequent causes of bowel obstruction in children aged 2 months to 5 years and is often the result of hyperthrophy of the Preyer patches, most likely secondary to viral infections. In approximately 20% of cases, an underlying disorder such as lymphoma, polyps, Meckel’s diverticulum or vascular malformations act as the lead point for intussusception. The classic triad is vomiting, colicky, severe abdominal pain and currant jelly stools but these signs are not always presents. Abdominal pain can occur at 15- to 20-minute intervals and become more frequent and severe over time. Children may behave normally and be free of pain between episodes but fever is common and mental status changes can occur. On physical exam, a sausage-shaped mass is sometimes palpable and the rectum must be examined for a positive stool Hemoccult test.
Plain abdominal radiographs can be performed to rule out contraindications for contrast enema and to evaluate for soft-tissue mass. It can show distended bowel loops with absence of gas (Figure 2). A target sign—two concentric radiolucent circles superimposed on the right kidney—or a crescent sign—a soft-tissue density projecting into the gas of the large bowel—also may be seen on abdominal radiographs of patients with intussusception.9 Ultrasound can show a bull’s eye, coiled spring or doughnut sign (Figure 3). A patient with intussusception should be NPO and receive IV hydration, with placement of a NG tube and transfer for surgical consultation and an air or barium enema study. The efficacy of administration of antibiotics before such a study has not been established but they sometimes are given because of the risk of perforation. Surgery is indicated when contrast enema is unsuccessful (Figure 4). In such a case, a patient should be admitted for observation because of the 2% to 5% risk of recurrence soon after reduction.



Incarcerated Hernias
Hernia is the protrusion of an organ or its fascia through the wall of the cavity that contains it. Umbilical hernia is most common, followed by inguinal and scrotal.10 Incarceration risk is greater during the first 6 months of life. Patients present with irritability and vomiting. On exam, an erythematous bulge is seen, which becomes more prominent with increased abdominal pres- sure. Reduction can be attempted by applying pressure along the proximal inguinal canal with one hand while “milking” gas or the content of the incarcerated bowel with the other hand for up to 5 minutes.11 If manual reduction is unsuccessful, a patient should be transferred for surgical evaluation. Ultrasonography can also be performed to confirm the diagnosis.
Hirschsprung’s Disease
Hirschsprung’s Disease is congenital absence of ganglion cells in the mesenteric and submucosal plexuses of the bowel, resulting in abnormal peristalsis of the aganglionic segment. In approximately 80% of cases, the rectosigmoid area is involved. The presentation may vary from complete obstruction at birth, with vomiting, abdominal distension and failure to pass meconium, to delayed passage of meconium and repeated episodes of constipation. Approximately 24% to 34% of patients may present with enterocolitis, explosive foul-smelling diarrhea, fever, vomiting, and abdominal pain and distension, which is the most severe and potentially lethal complication of Hirschprung’s disease.12 Such patients should be managed with volume resuscitation and broad-spectrum IV antibiotics to provide coverage against aerobic and anaerobic organisms. In children with a more classic presentation, a barium enema should demonstrate a transition zone, but the definitive diagnosis requires rectal biopsy.
Adhesions
Adhesive bowel obstruction can be seen in approximately 2% to 15% of patients who undergo laparotomy. Most cases occur within 3 months of the surgery and 80% within 2 years of the procedure. Patients present with emesis, abdominal distension, and irritability. Transfer should be performed for pediatric surgery consultation and nasogastric decompression.
Extra-abdominal Causes of Acute Abdominal Pain
Testicular Torsion
Testicular torsion occurs when the spermatic cord twists, compromising the blood supply to the testicles and scrotum. It can result from trauma or strenuous exercise, or the cause may not be obvious. Patients often report sudden testicular pain that may radiate to the lower abdomen and inguinal area, nausea and vomiting. On physical exam, the testicle is tender with a transverse orientation and elevation in the scrotum. Doppler ultrasound can distinguish between other diagnoses with normal or increased blood flow (epididymitis) and torsion (no flow). Prompt transfer to a hospital with a urologic service that can provide surgical exploration—preferably within 6 hours of the onset of pain—is required.
Ovarian Cyst and Ovarian Torsion
Ovarian cysts are uncommon in premenarchal patients, but females of reproductive age have the highest incidence of ovarian torsion.13 Pain from an ovarian cyst may result from bleeding into the cyst or rupture of a hemorrhagic cyst, causing peritoneal irritation. Rupture usually occurs preceding a menstrual period. Ultra- sound should be performed to document the size of the cyst and rule out tumors. Analgesia and proper follow up with gynecology is appropriate.
As with testicular torsion, patients with ovarian torsion present with sudden sharp pain that radiates to the ipsilateral groin and may be accompanied by nausea and vomiting. Doppler ultrasound is helpful in revealing the diagnosis, but definitive diagnosis is based upon surgical findings. Prompt gynecological consultation and surgery is required for definitive management. Complete blood count (CBC) may show anemia from hemorrhage, leukocytosis in ovarian necrosis, and electrolyte disturbances in patients who have severe vomiting.
Ectopic Pregnancy
Ectopic pregnancy is rare in the pediatric population but should be part of the differential diagnosis for all sexually active adolescents who present with acute abdominal pain. The classic symptoms include abdominal pain, vaginal bleeding and amenorrhea, but dizziness, vomiting, and symptoms of urinary tract infection (UTI) also may be present. Risk factors include previous ectopic pregnancy, pelvic inflammatory disease (PID), previous tubal ligation, use of an intrauterine device (IUD), infertility, and previous abortion. Ten to twenty percent of patients may present in shock. Pregnancy tests are very accurate and ultrasound usually shows an adnexal mass or blood in the cul-de-sac. ABCs should be the first step in management and a patient should be transferred for ob/gyn consultation and surgical management.
Pelvic Inflammatory Disease
Risk of PID is increased in patients who have recent insertion of an IUD, have multiple sexual part- ners, and use vaginal douches among other fac- tors. Patients with PID usually present with lower abdominal pain, vaginal discharge, urinary symptoms, and fever. On physical exam, vaginal/endocervical discharge may be abnormal or purulent and cervical motion and adnexal tenderness may be present. Blood work may show leukocytosis, and an elevated sedimentation rate and c-reactive protein (CRP) level. According to the Centers for Disease Control and Prevention, PID is confirmed if pelvic tenderness is associated with one or more of the following: acute or chronic endometritis or salp- ingitis with histologic evaluation of biopsy, demonstration of Neisseria gonorrhea or Chlamy- dia trachomatis in the genital tract, salpingitis visualized by laparoscopy or laparotomy, isolation of pathogenic bacteria in a clean speci- men from the upper genital tract, or inflammatory/purulent pelvic peritoneal fluid without a source.14 Evaluation should include cultures of cervix, urethra, rectum or urine for N. gonorrhea or C. trachomatis. Sexually active patients presenting with pelvic or lower abdominal pain with no other cause should be empirically treated with antibiotics for PID. For mild-mod- erate PID, ceftriaxone 250 mg IM once plus doxycycline 100 mg orally twice daily with or without metronidazole 500 mg twice daily for 14 days, or cefoxitin 2 g IM single dose and Probenecid 1g orally administered concurrently in a single dose plus doxycycline 100 mg twice daily with or without metronidazole 500 mg twice daily for 14 days can be given. Patients who are pregnant, have tubo-ovarian abscess, have failed oral therapy or have severe illness should be admitted for IV antibiotic therapy with cefotetan 2g every 12 hours or cefoxitin 2g IV every 6 hours plus doxycycline 100 mg every 12 hours.
Urinary Tract Infection
Fever may be the only manifestation of UTI in some children. Infants and young children may present with nonspecific symptoms such as vomiting, anorexia, diarrhea, lethargy, oliguria and failure to thrive. Older children may present with abdominal pain, flank or back pain, dysuria, or frequency. Urine culture is the gold standard for diagnosis, but urinalysis can be indicative of UTI.15 Urinary tract catheterization should be used to obtain urine from febrile infants. Children can be treated with oral antibiotic therapy such as a third-generation cephalosporin, trimethropim-sulfamethoxazole or amoxicillin-clavulanate (higher resistance rate). Antibiotic duration—a short course of 3 to 7 days vs a long course of 7 to 14 days—is controversial, but patients with febrile illness should be treated for at least 10 days.16 Infants younger than 2 months and patients with pyelonephritis, urinary tract obstruction or immunocompromise should be admitted for IV antibiotic therapy. Young children may require further follow up to evaluate for urinary tract abnormalities such as vesicoureteral reflux.
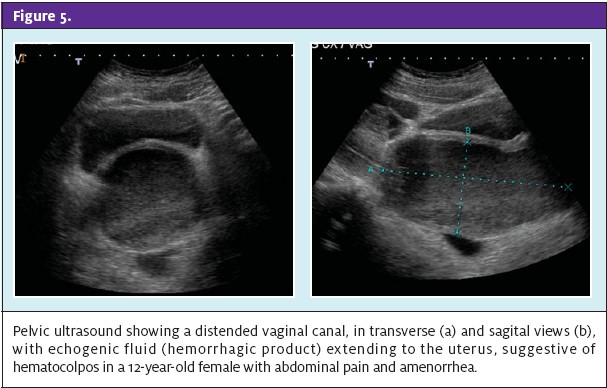
Hematocolpos
Hematocolpos is menstrual blood in the vagina. It is seen in adolescents who begin menstruation have retention of menstrual blood in the vagina because of an imperforate hymen. Patients usually complain of lower abdominal pain that some- times is associated with nausea and vomiting. On physical exam, a bulging, blue- domed area can be seen in the vaginal area. Pelvic ultra- sound can be performed to frequently associated with trauma, but also can be associated with drugs (steroids, thiazides, estrogen and L- asparaginase), systemic dis- eases (cystic fibrosis, and systemic lupus erythemaconfirm the diagnosis and to rule out hematometra (menstrual blood in the uterus) (Figure 5). An adolescent with hematocolpos should be transferred for gynecological evaluation and surgical repair.
Other Causes of Acute Abdominal Pain
Appendicitis
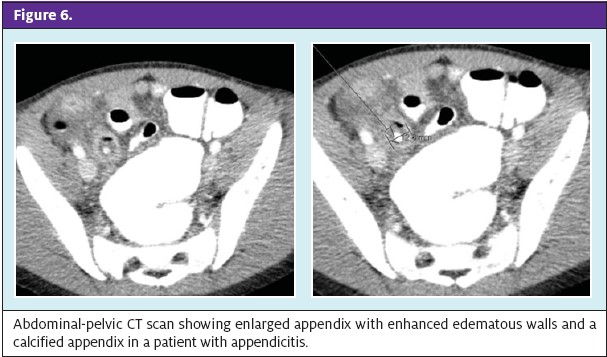
Appendicitis is most common in adolescents and relatively rare in patients younger than age 5 years, which leads to delayed diagnosis and higher rates of perforation.17 Most common symptoms include vomiting (85%-90%), pain (35%-77%), diarrhea (18%-46%), fever (40%-60%), and anorexia. In fewer than 50% of cases, localized right-lower-quadrant pain is noted. Vomiting is usually the first symptom, but progression of symptoms is somewhat difficult to verify. On physical exam, guarding, rebound tenderness, and other peritoneal signs may be present. Laboratory studies such as white blood cell count and CRP may support the diagnosis. Ultrasound and CT scan can be used when diagnosis is not clear (Figure 6). Patients with suspected appendicitis should be NPO, receive IV antibiotics, and be transferred for surgical consultation or repeated abdominal examinations if the diagnosis is still unclear.
Gallbladder Disease
Gallbladder disease is more common in adolescent females than in younger children. Hemolytic disease (sickle cell disease, spherocytosis and thalasemia), obesity and pregnancy are risk factors. Patients often present with right-upper-quadrant and epigastric pain that frequently radiates to the right subscapular area. Vomiting, fever, and jaundice may also be present. Laboratory studies such as a CBC, liver enzymes, and bilirubin levels can be performed. Ultrasound is the study of choice to evaluate for gallbladder disease. Cholecystitis is an inflammation of the gallbladder caused by gall- stones and should be treated with antibiotics, analgesia, a low-fat diet, and eventually cholecystectomy.
Pancreatitis
Pancreatitis is not common in the pediatric population, but can occur at any time during childhood. It is most frequently associated with trauma, but also can be associated with drugs (steroids, thiazides, estrogen and L- asparaginase), systemic dis- eases (cystic fibrosis, and tous), familial pancreatitis (autosomal dominant), infections (mumps) and anatomic abnormalities such as pan- creas duplication, ductal atresia or stenosis, and common duct stones. Patients usually complaint of mid epigastric abdominal pain that may be associated with nausea and vomiting. On physical exam, the abdomen may be distended, bowel sounds may be decreased, and tender- ness is found over the epigastric area. Elevated lipase and/or amylase levels (increase within 6 to 12 hours of onset and fairly rapid clearance from the blood) will help with the diagnosis.18 Lipase is more specific and some studies suggest that lipase elevations occur earlier and last longer than amylase elevations. Abdominal radiograph may reveal an epigastric sentinel loop or pancreatic cal- cifications. An enlarged, hypoechoic pancreas or a pseudocyst can be seen on ultrasound, but CT scan is the most important imaging test for diagnosis of pancreatitis and its abdominal complications. Patients should be transferred for admission and diet progression with enter- al feeds and, in very rare cases, for surgical management such as in the case of pancreatic necrosis.
Gastroenteritis
Gastroenteritis is more common in patients from low socioeconomic areas and with exposure to day care centers. Children younger than age 5 years may have 1 to 5 episodes per year but gastroenteritis can occur as often as 15 times per year in children in developing countries.19 Most episodes are viral and bacterial, and less likely caused by parasites. Symptoms (vomiting, diarrhea and abdominal pain) are usually brief and self-limited, lasting 3 to 7 days, but they may be prolonged by antimotility agents that cause intestinal stasis and prevent the protection afford- ed by enteric pathogens that result from active motility of the small intestine. Most patients with mild-to-mod-rate dehydration will respond to appropriate oral rehydration therapy. Patients with severe dehydration may have electrolyte abnormalities and need IV hydration and admission. Patients with intractable vomiting will also need to receive IV hydration. Rehydration should be started with isotonic solution such as normal saline or Ringer’s Lactate 20 mL/kg bolus. Further fluid management is beyond the scope of this article.
Constipation
Constipation is common in children and although there is not one simple definition, it can be considered as decreased stool frequency. A normal infant may pass stools 1 to 7 times a day.20 Toddlers can have 2 stools per day and children older than age 4 years may have 1 to 2 stools per day. Constipation is not a disease; it is a symptom of a problem such as cystic fibrosis, malnutrition, and Hirschsprung’s disease, among others.
On physical exam, fecal masses may be palpated on the left lower quadrant and a patient may have abdominal distension. On rectal exam, anal fissures may be seen and a distended rectum full of stool can be found (Figure 7). Treatment consists of disimpactation and evacuation of the stool remaining in the bowel, which can be accomplished by using hypertonic phosphate (Fleet) enemas. Oral laxatives such as lactulose, polyethylene glycol (Miralax), bisocodyl or senna can then be used. If a patient does not respond to such treatment, he or she should be referred for admission and disimpaction under physician supervision. Dietary changes should also be implemented to increase fiber consumption. In infants, sorbitol-containing juices such as prune or pear juice are an alternative.

Abdominal Masses
The tumors that most commonly present as abdominal masses include neuroblastoma, extragonadal germ cell tumors, hepatoblastoma and Wilms’ tumor.21 Neuroblastomas and hepatoblastomas are more common in children younger than age 2 years, whereas Wilms’ tumors, hepatocellular carcinoma, and ovarian germ cell tumors are more common in older children. Tumors are not a common cause of acute abdominal pain, but rather, present with progressing abdominal distension. Neuroblastomas initially manifest with watery diarrhea and some- times opsoclonus-myoclonus. Hematuria can be seen in patients with Wilms’ tumor. Patients with palpable abdominal masses should be transferred for further imaging and workup for definitive diagnosis. Specific workup and management is out of the scope of this article.
Uncommon causes of abdominal pain
Acute abdominal pain can be a symptom associated with different disease processes that generally have other distinguishing clinical features.22 Diseases will be mentioned as part of the differential diagnosis for abdominal pain but their management is out of the scope of this article. Some of the life-threatening diseases include diabetic ketoacidosis (usually also presenting with polyuria, polyphagia, and polydipsia), hemolytic uremic syndrome (bloody diarrhea, hemolytic anemia, thrombocytopenia, and acute renal injury), primary bacterial peritonitis (caused most commonly by Streptococcus pneumoniae in patients with nephritic syndrome), Henoch-Schönlein purpura (purpuric rash in lower extremities and buttocks, arthralgia, and renal disease), myocarditis, pericarditis, and pneumonia.
References
- Perry Abdominal Pain. In: Fleisher GR, Ludwig S, eds. Textbook of Pediatric Emergency Medicine. 7th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2010:584-588.
- Srevenson RJ and Ziegler Abdominal Pain Unrelated to Trauma. Pediatrics in Review. 1993;14;302-311.
- Neuman MI and Ruddy Emergent evaluation of the child with acute abdominal pain. Available at: http://www.uptodate.com/contents/emergent-evaluation-of-the-child-with- acuteabdominalpain?source=search_result&search=emergent+aval&selectedTitle=8%7E150 Accessed March 15, 2012
- Bailey B, Bergeron S, Gravel J, et Efficacy and impact of intravenous morphine before surgical consultation in children with right lower abdominal pain suggestive of appendici- tis: a randomized controlled trial. Annals of Emergency Medicine 2007; 50:371
- Green R, Bulloch B, Kabani A, et Early analgesia for children with acute abdominal pain.Pediatrics 2005; 116:978
- Clayton Focus on Diagnosis: Pediatric Abdominal Imaging. Pediatrics in Review 2010;31;506-510.
- Ross III Intestinal Obstruction in the Newborn. Pediatrics in Review. 1994; 15;338-347.
- Brandt Intestinal Malrotation. Available at: http://www.uptodate.com/contents/ intestinalmalrotation?source=search_result&search=malrotation+children&selectedTi- tle=1%7E45 Accessed March 15, 2012
- Kitagawa S and Miqdady Intussusception in children. Available at: http://www.upto- date.com/contents/intussusception-inchildren?source=search_result&search=intussuscep- tion&selectedTitle=1%7E96 Accessed August 22, 2012
- Singer Acute Abdominal Conditions. In: Strange GR, Ahrens WR, Schafermeyer R, et al. Pediatric Emergency Medicine: Just the Facts 2nd ed. The McGraw-Hill Companies; 2012: 42-45
- Ramsook C and Endoom Overview of inguinal hernia in children. Available at: http://www.uptodate.com/contents/overview-of-inguinal-hernia-in-children?source= search_result&search=incarcerated+hernias&selectedTitle=4%7E20 Accessed August 22, 2012
- Endoom EE AND Wesoon ED. Emergency complications of Hirschsprungs disease. Available at: http://www.uptodate.com/contents/emergency-complications-of-hirschsprung- disease?source=search_result&search=hirschprung&selectedTitle=2%7E55 Accessed August 22, 2012
- Growdon WB and Laufer MR. Ovarian and fallopian tube torsion. Available at: http://www.uptodate.com/contents/ovarian-and-fallopian-tube-torsion?source=see_link Accessed August 22, 2012
- Pelvic Inflammatory Disease ,Sexually Transmitted Disease Treatment Guidelines. Available at: http://www.cdc.gov/std/treatment/2010/pid.htm
- Feld LG and Matoo Urinary Tract Infections and Vesicourethral Reflux in Infants and Children. Pediatrics in Review. 2010;31;451-462
- Fitzgerald A, Mori R, Lakhanpaul M, Tullus Antibiotics for treating lower urinary tract infections in children. Cochrane Database Systematic Review. 2012 Aug 15;8:CD006857
- Holmes JA and DeLaney Pediatric Appendicitis. The Practical Journal of Pediatric Emer- gency Medicine. Volume 16, Number 11/November 2011; 129-137
- Verge Clinical manifestations and diagnosis of acute pancreatitis. Available at: http://www.uptodate.com/contents/clinical-manifestations-and-diagnosis-of-acute-pan- creatitis?source=search_result&search=pancreatitis&selectedTitle=1%7E150#H6 Accessed August 22, 2012
- Northurp RS and Flanigan Gastroenteritis. Pediatrics in Review. 1994;15;461-471
- Graham-Maar RC, Ludwig S, and Markowitz Constipation Fleisher GR, Ludwig S, eds. Textbook of Pediatric Emergency Medicine. 5th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2006:213-218
- Brodeur AE and Brodeur GM Abdominal Masses in Children: Neuroblastoma, Wilms tumor and Other Pediatrics in Review 1991;12;196-206
- Ferry GD Causes of acute abdominal pain in children and Available at: http://www.uptodate.com/contents/causes-of-acute-abdominal-pain-in-children-and-ado- lescents?source=search_result&search=causes+of+acute+abdominal&selectedTitle=1%7E15. Accessed November 23, 2011