Published on
Differential Diagnosis
- Anterior STEMI
- Grouped premature ventricular contractions
- Ventricular tachycardia
- Atrial flutter
- Atrial fibrillation with preexcitation
Diagnosis
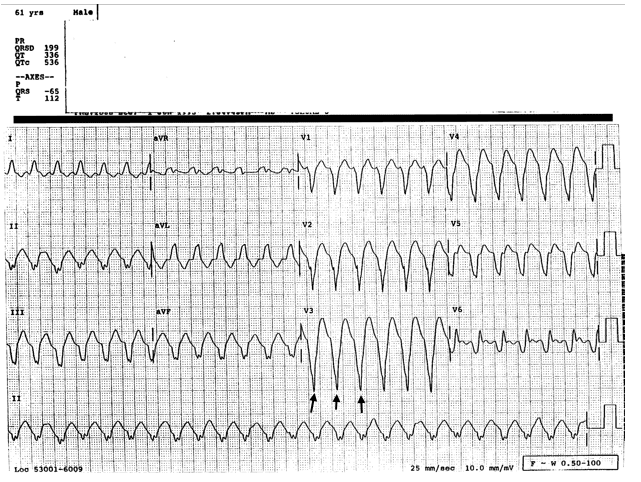
This patient was diagnosed with ventricular tachycardia (VT).
The ECG reveals a regular rhythm which is tachycardic, with a rate just above 150 bpm. There are no defined ST elevations across the anterior precordium, V3 and V4, so anterior STEMI is unlikely.
Grouped premature ventricular contractions (PVC) would be seen as a ventricular complex which occurs intermittently with sinus rhythm. Focusing on lead II (on the bottom of the ECG), we see that all the complexes here are the same, making a PVC or grouped PVCs unlikely.
Atrial flutter should show a sawtooth pattern, best seen in leads V1 and V2, and though the rate is close to 150 (commonly seen with atrial flutter), there are no “flutter” waves.
Atrial fibrillation is an irregularly irregular rhythm, but our patient’s rhythm is regular, so Afib is not occurring.
The ECG shows a wide complex, regular tachycardia without preceding P waves; this is VT.
Learnings/What to Look for
- VT is a wide complex tachycardia originating in the ventricles
- Monomorphic VT has complexes which originate from the same ventricular focus and are identical in appearance
- VT patients may be stable, as was our patient, or profoundly hemodynamically unstable
Pearls for Urgent Care Management and Considerations for Transfer
- Inquire about signs of ischemia such as chest discomfort, shortness of breath, diaphoresis, or dizziness
- Assess for hemodynamic instability such as hypotension, dizziness, or confusion
- VT is a true cardiac emergency and EMS should be emergently activated. While waiting, place the patient on a monitor and attempt to establish IV access
- Unstable patients require emergent cardioversion