Published on
Differential Diagnosis
- Atypical pneumonia
- Mediastinal widening
- Pneumothorax
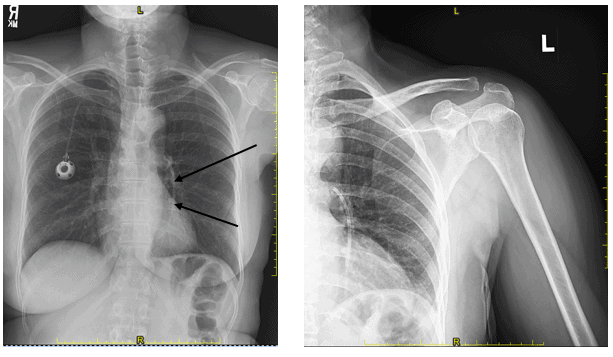
- Fractured infusion port catheter
- Wegener’s granulomatosis
Diagnosis
This patient has a fractured infusion port catheter which has migrated through the right atrium and right ventricle and lodged in the left main and lower lobe pulmonary artery.
Learnings/What to Look for
- This can occur in patients with inserted infusion ports inserted via subclavian route
- A fractured catheter can migrate to the superior vena cava, right atrium, right ventricle, pulmonary arteries, and internal jugular vein
- One reason is pinching of the catheter in the narrow space between the first rib and the medial end of the clavicle. Physical activity involving upper arms and the neck and increased intrathoracic pressure with coughing and vomiting are contributory factors
- Diagnosis is usually made on plain chest x-ray studies revealing a short length of the catheter attached to the port and a second “migrated” catheter fragment. Echocardiogram and CT could be used for more accurate anatomic assessment
Pearls for Urgent Care Management and Considerations for Transfer
- Other possible complications include cardiac perforation, cardiac arrhythmia, pulmonary embolism, sepsis, endocarditis, and superior vena cava thrombosis. Mortality among the untreated patients is high
- Treatment requires removal of the fractured port and vascular intervention for retrieval of the migrated fractured catheter
- If this is found incidentally and the patient is asymptomatic, phone consultation with the surgeon or interventional radiologist should be considered to facilitate timing and approach to removal
Images and Case courtesy of Dr. David Cohen, Teleradiology Specialists
A 58-Year-Old Female with a New Infusion Port and Shoulder Pain
1 2