Published on
The Resolution
Differential Diagnosis
- First-degree AV block
- Wolff-Parkinson-White syndrome (WPW)
- Anterior STEMI
- Brugada syndrome
- Third-degree heart block
Diagnosis
This patient has Brugada syndrome.
The syncope patient who is now “normal” is the classic urgent care encounter; typically all that is needed is a good history and physical and an ECG, looking for:
- Wolff Parkinson White
- Prolonged QT syndrome
- Brugada syndrome
- Hypertrophic cardiomyopathy
- Ischemia or arrhythmia
Regarding the “differential diagnosis” for the ECG above, the normal PR interval is 120-200 ms, with first-degree AV block being a duration longer than 200 ms, not present on this ECG. WPW is defined by a short PR, a delta wave, and a wide QRS complex—again, not present here. Could this be an anterior STEMI? Possibly…but the morphology of the ST segments is different than typically seen with a STEMI; plus, the leads with ST elevation are curious—anterior STEMI generally involves leads V3 and V4, not V1-3, and…in a patient without chest pain, shortness of breath or sweating, this would be a very unusual presentation indeed! The final possibility presented is third-degree heart block, where there is no conduction of the p waves to generate a QRS complex. Third-degree (complete) heart block will have a P wave rate unrelated to the rate of the QRS complexes. This ECG has p waves conducted and related to the QRS complexes; this ECG is not complete heart block. This ECG shows Brugada syndrome defined by a symptomatic patient with right bundle branch block (RBBB) or incomplete RBBB in leads V1 and V2 with concurrent ST segment elevation.
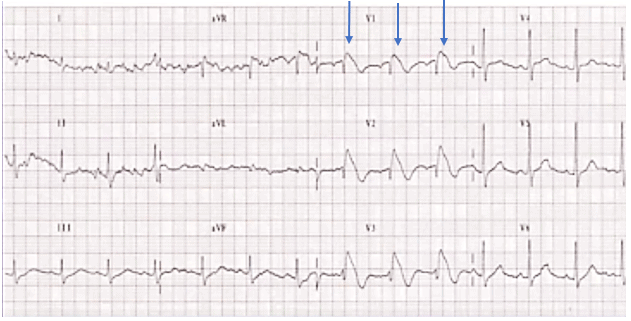
ST elevation with incomplete right bundle branch block (blue arrows)
Learnings/What to Look for
- Age of manifestation of Brugada syndrome is typically 30-40 years; it occurs in families
- Most patients are asymptomatic
- ECG will show incomplete RBBB in V1/V2 with ST segment elevation—saddle or cove type. These findings may be transient
- Brugada may be the culprit in up to 4%─5% of cardiac arrests
- Mortality is high without placement of an ICD, as there is a high risk of sudden cardiac death
Pearls for initial management and considerations for transfer:
- Perform an ECG in all syncope patients
- Many ECG machines are not programmed to read Brugada syndrome
- In the syncopal patient, look at the ECG specifically for Brugada syndrome, as well as for WPW, prolonged QT, HCM, and other serious arrhythmias, as well as ischemia
- Patients who have had a syncopal episode from Brugada are by definition symptomatic and either should be transferred to the ED by EMS or a plan determined after phone consultation with an electrophysiology cardiologist before the patient leaves the urgent care center
Acknowledgement: Image provided by Amal Mattu, MD.
