Published on
Differential Diagnosis
- Atrial fibrillation
- Multifocal atrial tachycardia
- Third-degree AV block
- Inferior STEMI
- Wolff-Parkinson-White syndrome (WPW)
Diagnosis
This patient has an inferior STEMI.
This ECG is normal sinus rhythm, with a P wave preceding each QRS. The normal PR interval is 120-200 ms; this PR is prolonged at 249, consistent with first-degree AV block, a generally benign finding. But that is only an incidental notation on this ECG, as there are major abnormalities in the ST segments inferiorly.
The inferior leads, II, III, and aVF, are limb leads which reflect changes at the inferior aspect of the heart, typically with blood supply from the right coronary artery. Further confirming the diagnosis is ST depression in lead aVL, called a reciprocal change, increasing the concern for inferior STEMI.
Atrial fibrillation is an irregularly irregular rhythm without defined p waves, not present on this ECG. Multifocal atrial tachycardia is often present in patients with COPD, and though irregular and fast, there is a p wave preceding each QRS. Third-degree AV block is confirmed with P waves which are not associated with the QRS complex, usually with a rate in the 30s. WPW is defined by a short PR segment (not present here) and a delta wave which is a gradual upsloping of the initial reflection of the QRS complex, often seen in the lateral precordial leads such as leads V5 and V6.
This ECG shows an inferior STEMI with reciprocal changes as well as first-degree AV block.
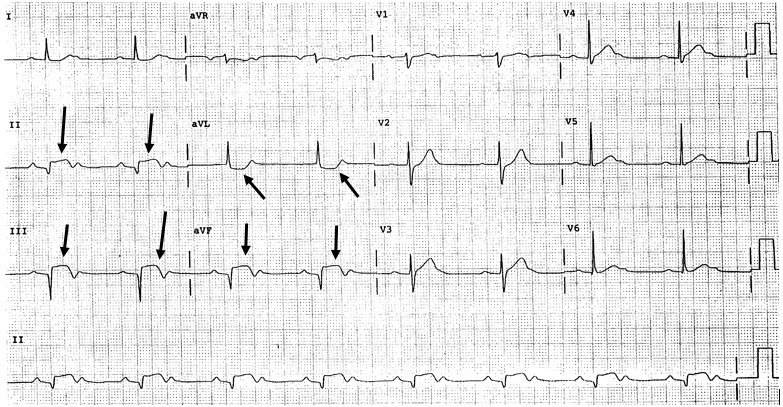
The downward facing arrows show the ST elevation indicating and inferior STEMI. The upward facing arrows highlight the reciprocal changes in lead aVL.
Learnings/What to Look for
- Patients with inferior ischemia or STEMI may present with epigastric pain, as opposed to chest pain
- In patients with epigastric pain, inquire about associated symptoms of ischemia/infarction such as diaphoresis, dyspnea, radiation, exertional discomfort, or vomiting
- Reciprocal changes will help to confirm the diagnosis of STEMI, but lack of reciprocal changes does not exclude the diagnosis of STEMI
Pearls for Urgent Care Management and Considerations for Transfer
- All patients presenting to the urgent care with STEMI will need emergent transfer to an ED with capability to perform percutaneous coronary intervention
- Inform EMS that the patient has a STEMI to facilitate rapid arrival
- While awaiting transfer the patient should be monitored, ACD at bedside (if available), and 1-2 IVs placed
- Provider-to-provider contact should optimally occur with the receiving facility and a copy of the ECG sent