Published on
Differential Diagnosis
- Hyperkalemia
- Hypercalcemia
- Acidosis
- Hyperthermia
- Digitalis toxicity
- Myocardial ischemia
Diagnosis
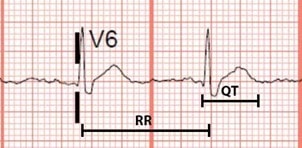
The ECG shows normal sinus rhythm at a ventricular rate of 75 bpm. The QT-interval, or the time between the start of the Q-wave and end of the T-wave, is shortened at 360 ms (nine small boxes at 40 ms each). This patient was diagnosed with hypercalcemia with shortened QT-interval.
Shortening of QT interval (QTC <360ms) and presence of Osborn J-waves are ECG findings commonly associated with hypercalcemia.1
The QT-interval varies based on the heart rate (lengthens at slower heart rates, shortens at faster heart rates) and should be corrected on this account. There exist several formulae for estimation of the corrected QT interval (QTC), of which the Framingham formula [QTC = QT + 154 x (1-RR)] may provide the most accurate estimation.2,3 In this case, the QTC is 391ms which is calculated as QT + 154 x (1- (60/HR)).
While other formulae exist for the estimation of lower bounds for normal QTC intervals, a cutoff of around 360 ms is reasonable for distinction of abnormally shortened QT.4 Though this patient’s ECG does not yet meet this threshold, Osborn J-waves are present. The Osborn J-wave is a positive deflection at the J-point (junction point between QRS complex and T-wave). Osborn J-waves can also be seen in other conditions including hypothermia.5,6

Finally, the ECG demonstrates some ST-segment changes, including elevations most pronounced in lead III. Shortening of the QT interval can result in a “high-takeoff” of the ST-segment, mimicking myocardial ischemia or infarction. This finding is unreliable, however, and ST-segment changes can only be attributed to hypercalcemia after appropriate exclusion of an acute myocardial infarction.7-9
Learnings/What to Look for
The identification of ECG changes associated with electrolyte derangements generally, and hypercalcemia specifically, is critical as these are manifestations of conduction abnormalities with a rare risk of progression to potentially fatal ventricular dysrhythmias (such as ventricular fibrillation).10 The ECG findings commonly associated with hypercalcemia are:1
- Shortening of QT interval (QTC <360ms)
- Presence of Osborn J-waves
- In addition to ECG, appropriate laboratory tests include hemoglobin, chemistry panel, and cardiac enzymes
Pearls for Urgent Care Management and Considerations for Transfer
- In addition to emergency department transfer for symptomatic hypercalcemia with associated ECG abnormalities, initial management may include isotonic volume expansion
References
- Diercks D, Shumaik G, Harrigan R, et al. Electrocardiographic manifestations: electrolyte abnormalities. J Emerg Med. 2004;27(2):153-160.
- Vandenberk B, Vandael E, Robyns T, et al. Which QT correction formulae to use for QT monitoring? J Am Heart Assoc. 2016;5(6):e003264.
- Sagie A, Larson M, Goldberg R, et al. An improved method for adjusting the QT interval for heart rate (the Framingham Heart Study). Am J Cardiol. 1992;70(7):797-801.
- Viswanathan M, Page R. Short QT circulation. Circulation. 2007;116(7):686-688.
- Otero J, Lenihan D. The “normothermic” Osborn wave induced by severe hypercalcemia. Tex Heart Inst J. 2000;27(3):316-317.
- Asbeutah A, Salem M. Electrographic Osborn wave in severe hypercalcaemia. Eur Heart J. 2019;3(4):1-2.
- Nishi S, Barbagelata N, Atar S, et al. Hypercalcemia-induced ST-segment elevation mimicking acute myocardial infarction. J Electrocardiol. 2006;39(3):298-300.
- Turhan S, Kilickap M, Kilinc S. ST segment elevation mimicking acute myocardial infarction in hypercalcaemia. Heart. 2005;91(8):999.
- Ashizawa N, Arakawa S, Koide Y, et al. Hypercalcemia due to vitamin D intoxication with clinical features mimicking acute myocardial infarction. Intern Med. 2003;42(4): 340-344.
- Kiewiet R, Ponssen H, Janssens E, Fels P. Ventricular fibrillation in hypercalcaemic crisis due to primary hyperparathyroidism. Neth J Med. 2004;62(3):94-96.
Acknowledgment: JUCM appreciates the assistance of ECG Stampede (www.ecgstampede.com) in sourcing content for electrocardiogram-based cases for Insights in Images each month.